Collision with terrain
Far West Helicopters Ltd.
Bell 206B (Helicopter), C-FWHF
Deception Mountain, British Columbia, 3.6 nm SSE
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
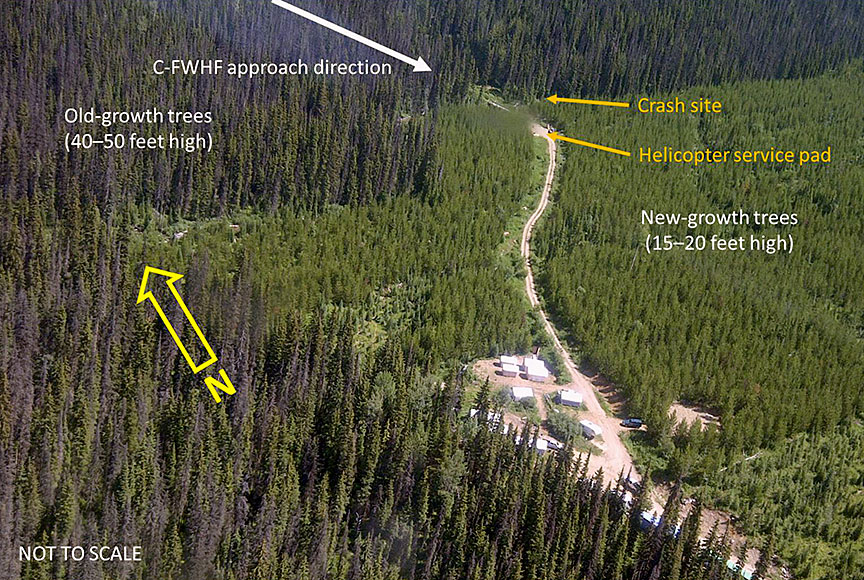
The Far West Helicopters Ltd. Bell 206B helicopter (registration C-FWHF, serial number 1525) was returning to a remote base camp situated 3.6 nautical miles south-southeast of Deception Mountain, British Columbia, at an elevation of 4100 feet above sea level. The flight took place during daylight hours, with only the pilot on board. At 1358 Pacific Daylight Time, as the helicopter was approaching a service pad, the pilot perceived a power fluctuation. In response, the pilot conducted a straight-in approach to the service pad and applied cyclic and collective control inputs to remain clear of trees. The helicopter pitched up to an extreme nose-high attitude. There was a popping or banging sound, and several pieces of debris separated from the helicopter. The helicopter began to descend and rotate to the left, eventually striking terrain approximately 200 feet northeast of the service pad. Base camp personnel witnessed the event and called 911. The pilot was seriously injured and was evacuated by air ambulance. The helicopter was substantially damaged. The emergency locator transmitter activated. There was no post-impact fire.
Factual information
History of the flight
The Far West Helicopters Ltd. Bell 206B helicopter (registration C-FWHF, serial number 1525) was operating in support of mineral exploration, out of a base camp approximately 3.6 nautical miles (nm) south-southeast of Deception Mountain, British Columbia. The camp, equipped with a helicopter service pad and fuelling equipment, was at an elevation of 4100 feet above sea level in a forest of new-growth trees, in an area that had previously been clear-cut (Figure 1).
The pilot had been operating out of the base camp for 10 days prior to the accident. During a flight on the second day of operations—approximately 16 flying hours before the accident occurred—the pilot had encountered fluctuations of gas-producer-turbine speed (N1) and main-rotor speed (NR), accompanied by shaking of the helicopter. He had increased the NR using the engine governor revolutions per minute (rpm) switch,Footnote 1 and the problem had abated.
Typically, the pilot started with a fuel load of 45 gallons and planned to refuel when no less than 20 gallons remained. He had performed the pre-flight inspection earlier in the day and had noted that the fuel sumps were free of water.Footnote 2
On the day of the accident, the first flight began at 1330.Footnote 3 On the second flight, the pilot flew 2 prospectors up the mountain to the drill site. At approximately 1350, the helicopter departed the drill site to return to the base camp, where the pilot intended to refuel and pick up slinging equipment. The pilot radioed the base camp at 1357 and stated that he was inbound to the service pad.
The helicopter approached from the north, over old-growth trees on terrain that descended toward the service pad, which was surrounded by new-growth trees. The pilot then intended to execute a 180° turn back to the service pad.
The pilot elected to cross a low ridge on a more direct route to the base camp area to avoid patchy fog present along his usual route. At 1358, as the helicopter flew over the low ridge, the pilot perceived a fluctuation in engine power. The pilot abandoned the 180° turn and flew directly to the service pad. He applied aggressive cyclic and collective control inputs to remain clear of the trees and to position the helicopter for a straight-in approach. The helicopter pitched up to a steep nose-high attitude. There was a popping or banging sound, and several pieces of debris separated from the helicopter. The helicopter began to lose altitude and rotate to the left. The pilot lowered the collective lever and reduced the throttle to idle in an attempt to establish autorotation and manoeuvre the helicopter to a landing.
After about 2 complete rotations during the descent, the helicopter collided with terrain among the older-growth trees. It came to rest straddling a small boulder-strewn creek, approximately 200 feet from the service pad. The emergency locator transmitter activated and emitted signals on 121.5 megahertz (MHz) and 406 MHz that were detected by overflying aircraft and Cospas-Sarsat,Footnote 4 respectively.
Base camp personnel who had witnessed the collision alerted emergency services via a 911 call and then made their way to the crash site. When they arrived, the pilot was still inside the aircraft, its fuel cell was leaking, and its engine was still running. The pilot was seriously injured but conscious and was still wearing the 4-point seat belt and shoulder harness; he was not wearing a helmet.
Base camp personnel removed the helicopter's left-side doors and doorpost and extricated the pilot from the wreckage. They moved him to the bank of the creek to wait for emergency services personnel and then cut a trail to the crash site to facilitate stretcher access.
The helicopter's collective lever had broken during the crash. Due to the integrated twist-grip throttle, it was not possible to shut down the engine by closing the throttle. The engine was eventually shut down, roughly 30 minutes after the crash. Base camp personnel had to restore electrical power to the aircraft to move the electrically driven fuel shut-off valve to the closed position. There was no post-impact fire. An air ambulance transported the pilot to the hospital.
Injuries
The pilot sustained severe injuries.
Damage to aircraft
The helicopter was substantially damaged due to the collision with terrain (Figure 2).

Other damage
An unknown quantity of jet fuel leakedFootnote 5 from the helicopter's ruptured fuel cell. The majority of the leaked fuel drained directly into the small, fast-running creek beneath the wreckage.
Personnel information
Records indicate that the pilot was certified and qualified for the flight in accordance with existing regulations. The pilot held a valid airline transport pilot licence—helicopter with a Category 1 medical certificate that was valid until 01 July 2017. He held type ratings on the Bell 206B and 5 other helicopter types.
Before beginning his employment with Far West Helicopters Ltd. in May 2016, the pilot had accumulated 11 265 hours of flight time, 9067 of which had been as pilot-in-command and 850 of which had been on the Bell 206B. From 21 May 2016 to the time of the accident, he had accumulated approximately 54 hours of flight time on C-FWHF.
Since the pilot's arrival at the base camp on 24 August 2016, he had carried out 7 to 9 flights per day. These flights amounted to roughly 1.1 to 2.9 daily flying hours, for a total of about 21 hours until the day of the accident.
Limited data were available regarding the quality of the pilot's rest. Shortly after arriving at the base camp, the pilot had insisted on private quarters, and the base camp manager had therefore arranged for a separate cabin. In the 10-day period of the pilot's stay at the base camp, his work schedule had afforded opportunities for a period of rest following each day of flying, and sufficient time for sleep had been available to him; on occasion, camp activities and issues with the accommodations interrupted his rest. However, insufficient additional information was available regarding the pilot's sleep history to allow for a full fatigue analysis.
Aircraft information
Records indicated that the helicopter was certified, equipped, and maintained in accordance with existing regulations. C-FWHF was manufactured in the United States in 1974, and Far West Helicopters Ltd. had imported it to Canada in 2012. Following an extensive rebuild, the helicopter had entered service in November 2015. Since then, it had accumulated roughly 154 hours of flight time, 40 of which were after the 100- and 200-hour inspections performed in June 2016.
The helicopter had no known deficiencies before the occurrence flight, and it was being operated within its weight-and-balance and centre-of-gravity limits. No record of any N1 or NR fluctuations was entered in the aircraft journey logbook, and no related troubleshooting or maintenance action was carried out.
Satellite tracking system
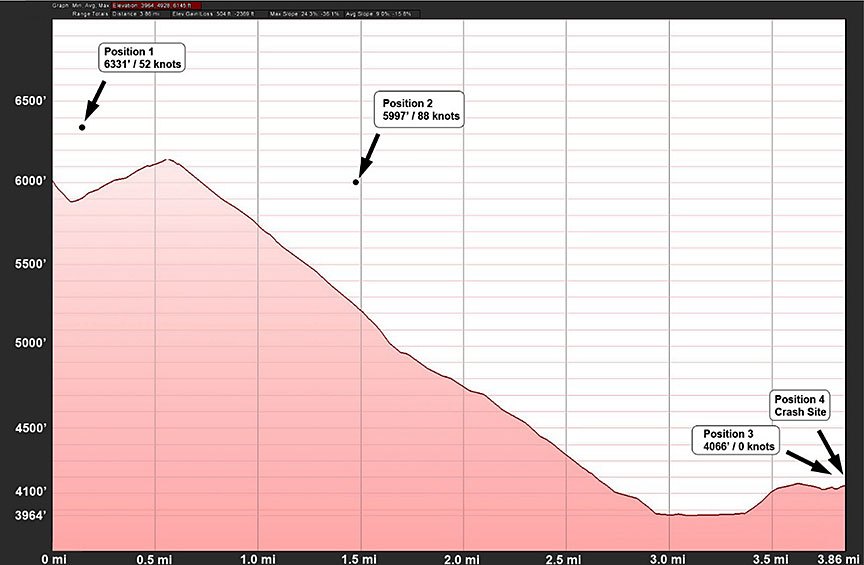
The helicopter was equipped with a satellite tracking system that uploaded the following information to a web-based application at intervals of approximately 2 minutes:
- time;
- latitude and longitude;
- ground speed (in knots);
- track (in degrees); and
- altitude (in feet above sea level).
The system had recorded 4 data points during the accident flight (Figure 3).
Meteorological information
Flight operations on the day of the accident were delayed by fog at the higher elevations where the prospectors were working. Patchy fog was present along a creek in a valley on the pilot's usual route. However, conditions at the base camp were clear, and the wind was calm. Weather conditions were not contributory to the accident.
Wreckage and impact information
Following a descent through trees, the helicopter collided with the terrain on either side of a small, boulder-strewn creek. Its main-rotor blades exhibited damage that was consistent with a very low rotor rpm at the time of ground contact. Red paint transfer resulting from contact with the vertical stabilizer was evident on one blade. The rotating components of the upper swashplate assembly had contacted the surrounding cowling. Scrapes were evident on the cowling, and some metal had been torn away.
Boulders supported the fore and aft sections of the fuselage, which spanned the creek and had collapsed downward near the doorposts and pilot seat. The aft landing gear cross-tube had penetrated the fuel-cell cavity, causing the fuel cell to rupture and leak. An undetermined quantity of fuel remained trapped in the folds of the cell.
The aft section of the tail boom had separated and lay in the creek, with the tail-rotor gearbox and tail rotor still securely attached.
The pylon plate and static stop were broken in several places and had separated from the roof. The isolation mount remained attached to the fuselage roof and drag link; however, the drag link had separated from the bottom of the main-rotor transmission.
The power lever on the fuel control unit was in the idle position. When the fuselage had collapsed, it had bent the flight-control tubes in the vertical tunnel and locked them in position. The collective lever had broken away at the casting, and the twist-grip throttle was in the idle position.
The helicopter was equipped with an engine auto-relight system. Because base camp personnel had moved some switches on the instrument panel during attempts to shut down the engine after the accident, the pre-impact position of some of the switches and controls could not be determined with certainty.
The wreckage was transported to the Transportation Safety Board of Canada (TSB) facility in Richmond, British Columbia.
Examination of components
The engine (Rolls Royce model 25O-C20B, serial number CAE 821362) and related accessories were sent to an engine overhaul facility, where they were examined under the supervision of TSB investigators and representatives of the engine and helicopter manufacturers. No pre-impact anomalies were noted on the engine or its accessories that would have precluded normal operation. However, the engine-mounted anti-ice valve was missing a small fibre washer from the end of the valve shaft. The missing washer meant that bleed air was continuously heating the compressor inlet. In effect, the engine anti-ice system would have been operating continuously, resulting in a slightly increased turbine outlet temperature and a corresponding slight reduction in available power.
Due to the post-accident condition of the engine, it was not possible to run it in an engine-testing facility. The engine was disassembled, and no anomalies were noted. The engine accessories underwent individual inspection and bench tests prior to installation on a serviceable exemplar engine. During the on-engine testing, the anti-ice valve was operated manually while the power demand from the engine was suddenly increased. All engine accessories performed satisfactorily during the bench and on-engine test procedures.
The main-rotor transmission, freewheel unit, and tail-rotor gearbox all rotated freely.
The following items were sent to the TSB Engineering Laboratory for further examination:
- freewheel unit
- pylon drag-link attachment hardware
- main driveshaft and bolts
- isolation mount
- hydraulic pump
No defects that could have contributed to the occurrence were noted in those items.
Spike knock
The fuselage of the Bell 206B is suspended from the main-rotor transmission by 2 A-frame pylons. Spherical bearings allow the pylons, and hence the main-rotor transmission and mast, to move in relation to the fuselage, with the motion dampened by the isolation mount. Main-rotor thrust and dynamic forces normally maintain the main-rotor transmission and fuselage in alignment; however, certain manoeuvres can cause unbalanced pylon motion. This phenomenon, known as pylon whirl, can lead to spike knock, which is described as follows:
Footnote 6Compressor stall
A compressor stall is defined as
Footnote 7This condition can cause the normal airflow through the engine's compressor to slow, stop, or even reverse direction. The latter is usually referred to as a compressor surge. A number of conditions can cause compressor stalls. Two conditions of interest to this investigation were
- interrupted airflow at the compressor inlet, resulting from turbulence or aircraft manoeuvres; and
- sudden engine acceleration that can cause too much fuel to be delivered, resulting in excessive back pressure in the combustion chamber.
A compressor stall may occur in degrees of severity, ranging from a pulsing sound or a pop to, in the case of a compressor surge, a loud bang.
Helmet use
Although the pilot usually wore a helmet when passengers did so or when performing slinging or long-line work, his helmet had been left in the base-camp cabin on the day of the accident and was not worn. He was not required by the operator to wear a helmet, and helicopter pilots are not required by regulation to wear head protection.
Studies of helmet usage
The head is the second most frequently injured region of the body in survivable helicopter crashes.Footnote 8 According to research examining U.S. army helicopter accidents, the risk of fatal head injuries may be as high as 6 times greater for helicopter occupants not wearing head protection.Footnote 9 The immediate effects of non-fatal head injuries range from momentary confusion and inability to concentrate to full loss of consciousness.Footnote 10 Incapacitation can compromise a pilot's ability to escape quickly from a helicopter and to assist passengers in an emergency evacuation or survival situation.
In 1988, the National Transportation Safety Board reviewed 59 emergency medical services (EMS) aviation accidents occurring from 11 May 1978 to 03 December 1986.Footnote 11 The study's findings led to the issuance of 2 National Transportation Safety Board recommendations aimed at reducing the risk of injury and death in survivable accidents:
- Safety Recommendation A‑88-009, calling on the FAA to require that EMS helicopter flight crew and medical personnel wear helmets and other protective clothing and equipment
- Safety Recommendation A‑88-014, urging the American Society of Hospital-Based Emergency Aeromedical Services to encourage its members to provide protective clothing and equipment, including helmets, to medical personnel who routinely fly EMS helicopter missions
In 1998, Transport Canada's Safety of Air Taxi Operations Task Force (SATOPS) recognized the safety benefits of protective head equipment, issuing the following recommendation in its final report:
Footnote 12 Footnote 13To industry, the task force directed the following additional recommendation:
Footnote 14The TSB has documented a number of occurrencesFootnote 15 in which the use of head protection likely would have reduced or prevented the injuries sustained by the pilots involved, as well as occurrences in which the use of head protection reduced or prevented injuries.
In recognition of the benefits of head protection, the following resolution was passed by the Board of Directors of the Helicopter Association of Canada (HAC) on 27 June 2011:
Footnote 16HAC also pointed out, however, that certain pilot/aircraft type configurations may preclude safe helmet use.Footnote 17
Crash-resistant fuel systems
The TSB has investigated a number of helicopter accidents in which fuel was spilled on impact (Appendix A). The subsequent fuel-fed post-impact fires resulted in serious injuries or fatalities in otherwise survivable crashes.
In 1994, new standards for fuel-system crash resistance for transport category rotorcraft were adopted into both the Canadian Aviation RegulationsFootnote 18 and the United States Federal Aviation Regulations.Footnote 19 The standards are applicable to helicopters that received type certificates after 1994. Helicopter models that received a type certificate prior to 1994 are not required to comply with these regulations, even if the helicopters were manufactured after 1994.
A recent update by the U.S. Federal Aviation Administration's Rotorcraft Occupant Protection Working Group included information comparing occupant survivability in accidents involving helicopters equipped with crash-resistant fuel systems (CRFSs) to those without CRFSs. The update also reviewed statistics comparing the percentages of helicopters equipped with and without CRFSs. At the end of 2014, CRFSs were found to be incorporated in 16% of the U.S. rotorcraft fleet. Accidents from 1995 to 2015 involving 58 CRFS-compliant rotorcraft were reviewed. The accidents were rated for impact severity (none, minor, moderate, severe, or extreme). There were no reports of fuel-spillage fires up through the severe level. Fuel spillage fires occurred in 3 of the 9 extreme-level crashes. However, none of the extreme-level crashes were survivable.Footnote 20
Bell Helicopter first introduced CRFSs to its commercial fleet in 1979, beginning with the Bell 222. Over the next few years, CRFSs were embodied on the production line for most of the commercial fleet, including the Bell 206B. All variants of the Bell 206B manufactured after 1983 were equipped with CRFSs at the factory. Bell Helicopter has offered a CRFS modification kit for the Bell 206B helicopter since the early 1990s.
One component of a compliant CRFS is a crashworthy fuel cell. Crashworthy fuel cells for some helicopter models are available as aftermarket modification kits. Although embodiment of such a modification may not fully comply with the current CRFS standards, installing crashworthy fuel cells reduces the probability of fuel spillage in the event of an accident. Non-crashworthy fuel cells are no longer procurable through Bell Helicopter for the Bell 206B helicopter.
C-FWHF was manufactured in 1974. It was not equipped with a CRFS or a crashworthy fuel cell, nor was it required to be by regulation.
TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP223/2016 – Engine & Transmission Analysis
- LP299/2016 – Freewheel and Tach Signal Generator Analysis
- LP121/2017 – Hydraulic Pump Input Shaft Examination
- LP156/2017 – Material Analysis – Bolts and Studs
- LP171/2017 – Terrain Evaluation
Analysis
General
The pilot was certified and qualified for the flight. Incomplete data precluded a full fatigue analysis; however, pilot fatigue was likely not a factor in the occurrence.
The investigation revealed no pre-existing issues with the helicopter's flight controls that would have contributed to the accident. It was determined that there was sufficient fuel on board, given that the engine continued to run after the impact.
The analysis will examine the power fluctuation, the pitch-up manoeuvre and subsequent landing attempt, and the survival aspects of the accident.
Power fluctuations
Although gas-producer-turbine (N1) and main-rotor (NR) speed fluctuations had occurred on the pilot's second day of operation, no maintenance action had been carried out.
Post-accident examination of the engine revealed no pre-impact anomalies, and all accessories were successfully test-run on an exemplar engine. A fibre washer was missing from the anti-ice valve, which would have led to continuous operation of the engine anti-ice system. The resulting increase in turbine outlet temperature would have marginally affected the maximum power available. However, the cause of the perceived power fluctuation on the occurrence flight could not be determined.
Pitch-up manoeuvre
Because of patchy fog along the pilot's usual route, the pilot decided to cross over a low ridge before turning 180° for a landing. This route took the helicopter over older-growth trees directly toward the service pad, which was partially obscured by new-growth trees. After perceiving a power fluctuation, the pilot abandoned the 180° turn and flew directly to the service pad using aggressive control inputs to position the helicopter for a straight-in approach.
The attempt to reduce the rate of descent and airspeed with aggressive cyclic and collective control inputs caused the helicopter to pitch to an extreme nose-up attitude. It is likely that the extreme attitude led to the onset of pylon whirl and spike knock, resulting in contact between the rotating swashplate components and the cowling; this was consistent with the reported popping or banging sound. The torn and missing metal in the cowling was likely the debris that had separated from the helicopter.
There was an alternate potential explanation for the sound, but it was considered less likely: from a relatively low power state, the application of power through aggressive collective control input, in combination with the extreme nose-up attitude, may have induced a compressor stall.
The pilot lowered the collective and reduced the throttle to idle in an attempt to establish autorotation; however, there was insufficient height to conduct a successful autorotation to the service pad, and the helicopter collided with the terrain.
Survival aspects
The pilot was held in place during the crash because he was using the available restraint system. The considerable vertical deceleration forces were attenuated by the deformation of the pilot's seat and the downward collapse of the fuselage into the creek. The pilot was not wearing a helmet. During the crash, the cockpit broke open and collapsed downward, exposing the pilot's head to potential impacts. Other injuries prevented the pilot from exiting the wreckage on his own; however, head injuries alone could have compromised survival in the event of a post-impact fire. Helicopter pilots who do not wear helmets are at increased risk of incapacitation, serious injuries, or loss of life in the event of an accident.
The landing-gear cross-tube ruptured the fuel-cell compartment, allowing fuel to leak from the cell. The live electrical system and the running engine were potential sources of ignition. However, the fuel leaked directly into the creek, and the fast-flowing water carried it from the crash site, preventing the possibility of a fuel-fed post-impact fire.
Crashworthy fuel cells are available for some helicopter models and, although they may not make the helicopter fully compliant with current standards, can substantially reduce the probability of fuel-fed post-impact fires and of subsequent injuries and fatalities.
If helicopters are not equipped with crashworthy fuel cells, the risk of injury or death due to post-impact fire is increased.
Findings
Findings as to causes and contributing factors
- The cause of the perceived power fluctuation could not be determined.
- After perceiving a power fluctuation, the pilot abandoned the 180° turn and flew directly to the service pad using aggressive control inputs to position the helicopter for a straight-in approach.
- Attempts to reduce the rate of descent and airspeed caused the helicopter to pitch to an extreme nose-up attitude.
- It is likely that the extreme attitude led to the onset of pylon whirl and spike knock, resulting in contact between the rotating swashplate components and the cowling.
- There was insufficient height to conduct a successful autorotation to the service pad, and the helicopter collided with the terrain.
Findings as to risk
- Helicopter pilots who do not wear helmets are at increased risk of incapacitation, serious injuries, or loss of life in the event of an accident.
- If helicopters are not equipped with crashworthy fuel cells, the risk of injury or death due to post-impact fire is increased.
Safety action
The Board is not aware of any safety action taken following this occurrence.
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – TSB helicopter accident investigations citing fuel spillage
| Occurrence number | Post-impact fire? | Fatalities | Injuries | Comments |
|---|---|---|---|---|
| A00W0105 | Yes | 1 | 0 | The pilot succumbed to injuries sustained in the post-impact fire. |
| A01P0003 | No | 0 | 2 | The fuel tanks ruptured. |
| A01Q0139 | Yes | 3 | 0 | The pilot was fatally injured on impact. The passengers survived the impact, but later succumbed to their injuries. |
| A02A0098 | No | 0 | 1 | The injured pilot was unable to egress. |
| A05P0184 | Yes | 0 | 1 | The fuel cell compartments ruptured. The injured pilot required assistance to egress the burning wreckage. |
| A08P0035 | No | 1 | 1 | The pilot received fatal injuries and 1 passenger was seriously injured. The 8 remaining passengers were not injured. A fuel leak into the cabin was stopped by an uninjured occupant. |
| A09Q0210 | No | 0 | 2 | One occupant required assistance to egress the wreckage. |
| A09Q0131 | Yes | 2 | 0 | The persons who arrived at the site a few seconds after the accident were unable to control the flames that engulfed the helicopter, and therefore could not rescue the occupants. |
| A09W0146 | Yes | 2 | 1 | The pilot was ejected from the helicopter and survived; the 2 passengers were fatally injured. |
| A12P0008 | No | 1 | 0 | The fuel tank ruptured. |
| A13Q0021 | No | 0 | 3 | Two unconscious pilots, whose clothes were soaked in fuel, were removed from the wreckage by the pilot observer. |
| A14Q0060 | No | 0 | 2 | Approximately 220 L of fuel were spilled. The pilot assisted the observer out of the wreckage. |
| A15A0045 | No | 1 | 2 | Approximately 240 L of fuel were spilled. |
| A15C0146 | Yes | 2 | 0 | The fuel tank ruptured. The impact forces were not survivable. |
| A15Q0126 | Yes (extinguished) | 2 | 3 | The fuel tank ruptured. On-site personnel extinguished the post-impact fire. |