Employee fatality
Canadian National Railway Company
Remote control locomotive system
Extra yard assignment Y1XS-01
Melville, Saskatchewan
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 22 December 2017, at about 1800 Central Standard Time during hours of darkness, a Canadian National Railway Company (CN) foreman and a helper were performing switching operations at CN’s Melville Yard in Melville, Saskatchewan. The foreman was operating extra yard assignment Y1XS-01 using a remote control locomotive system (RCLS) when the foreman became pinned between the assignment and the lead car of an uncontrolled movement while applying a hand brake. The foreman received fatal injuries. There was no derailment and no dangerous goods were involved.
The movement consisted of 3 open-top hopper cars loaded with ballast. The foreman had kicked these cars up an ascending grade toward a connecting track, but at too slow a speed for them to reach it. Without sufficient speed, the cars stalled on the grade and began to roll back uncontrolled. The foreman ran to and boarded the lead car and applied a hand brake, but the braking efficiency of the hand brake was compromised. As a result, the uncontrolled movement did not stop or slow down, reducing the opportunity and time available for the foreman to get out of harm’s way.
The investigation identified a number of safety deficiencies described below.
Crew communication
The CN General Operating Instructions require job briefings to ensure that all crew members understand the work that is to be done.
In this occurrence, although the foreman and helper held 2 job briefings, several elements of the plan were not communicated and/or coordinated effectively:
- Each switching move was not discussed during the job briefings or as the work progressed.
- The helper believed that the foreman would be shoving the 3 cars into the destination track and was unaware that the foreman intended to kick them.Footnote 1 Thus the helper was positioned about 50 feet along the track, beside the location where the 3 cars were to be placed and was not in a position to intervene when the 3 kicked cars began to roll back.
- The helper’s view of cars being kicked was obstructed by cars standing in an adjacent track.
- There was no radio communication or discussion before the cars were kicked.
The crew members’ reserve, inexperience in working together, and relative inexperience in their roles on the day of the accident likely contributed to their infrequent communication during their shift.
Crew training and experience
The training provided to qualified conductors is generally sufficient to operate the RCLS equipment; however, it does not necessarily provide the experience needed when performing tasks that rely upon judgment, such as kicking cars up a grade. Given the multiple variables involved, the development of the judgment needed to carry out these types of movements effectively and safely under a variety of conditions can only be gained through on-the-job experience after training has been completed.
At Melville Yard, it was common practice for a foreman to control all yard movements, even though both crew members were equipped to operate RCLS. This practice limited the amount of operating experience that helpers received, potentially affecting their progress toward becoming competent and safe RCLS switching foremen. Moreover, the pairing of junior employees for yard assignments meant that a transfer of knowledge through coaching was limited.
The foreman had about 3 years of railway experience working with 2 different companies; however, she had limited recent opportunity to be the foreman of a 2-person crew while operating an RCLS locomotive. This experience may not have been adequate to develop the skills and judgement necessary to safely kick cars up a grade consistently. The foreman’s limited experience in operating an RCLS during switching operations likely contributed to the development of an inadequate plan and the attempt to kick the 3 cars at too slow a speed in an area of known ascending grade.
Pairing of inexperienced remote control locomotive system operators
In the railway industry, conductors are assigned the task of being RCLS operators, particularly in rail yards across the country. Conductors are generally unionized positions that are governed by collective agreements between the employer and the union. In most cases, local yard assignments are posted for bidding each week. After the employees submit their bids, the positions are awarded based on seniority in accordance with the collective agreement.
Some of the posted positions are favoured owing to the rate of pay, days off, and hours of work. Typically, the evening shifts and the night shifts are considered the least desirable, and yard positions in particular are normally regarded as the least desirable because the pay rates for these positions are the lowest. If no bids are received for a specific position, the position is awarded to the employee with the least seniority.
As extensive employee turnover has been occurring in the railway industry in the past few years, it is not unusual for the 2 most junior, and least experienced, employees at a terminal to be working together in yards, particularly during the evening and night shifts. The pairing of inexperienced crew members is not uncommon in the Canadian railway industry.
Since 2007, the TSB has completed 6 investigations (including this occurrence) that highlight the risks associated when conductors with low levels of experience are paired together to carry out yard assignments. The TSB determined that the relative inexperience of the RCLS operators (conductors) contributed to these occurrences through insufficient knowledge to make effective decisions with respect to planning and train handling. Further, the TSB determined that the practice of pairing junior employees together for yard assignments meant that the coaching and mentoring needed to develop effective judgment for train handling were not being provided.
While an operating employee must demonstrate the competencies required to perform work as a qualified foreman, there is no company or regulatory requirement outlining the time or experience required before a conductor assumes the role of yard foreman. These roles are tied to a collective agreement for unionized staff. Consequently, the crew member with more seniority at the railway would typically be assigned the role of foreman, regardless of the employee’s experience with the task.
Given the ongoing employee turnover in the railway industry and the potential adverse outcomes when inexperienced RCLS operators are paired together working in yards, the Board is concerned that, without additional mitigation, inexperienced RCLS operators will continue to be paired together in yards with a commensurate risk of ongoing adverse outcomes.
Reducing the frequency and associated risks of uncontrolled movements while switching without air
In this occurrence, a foreman was controlling a yard assignment using an RCLS while switching without air (i.e., without using air brakes) in Melville Yard. During switching operations, the foreman received fatal injuries while attempting to stop an uncontrolled movement by applying a hand brake.
The TSB classifies uncontrolled movements into 1 of 3 broad causal categories: loss of control, switching without air, and securement. Since 2016, the TSB has completed 3 investigations,Footnote 2 including this one, involving uncontrolled movements that occurred in yards while switching without air.
Switching without air occurs when a movement is switching with the use of the locomotive independent brakes only, with no air brakes available on the cars being switched or kicked. The vast majority of these incidents occur in yards.
In a report on a similar occurrence (TSB Railway Investigation Report R16W0074), the Board issued a safety concern that the current defences were not sufficient to reduce the number of uncontrolled movements and improve safety.
Between 2009 and 2018, 562 unplanned/uncontrolled movements occurred. There has been an upward trend during this 10-year period. The average increase per year for all categories was 1.67 occurrences, with 86% of the overall increase associated with switching without air. Of the 185 occurrences involving switching without air, 70 (38%) occurred as a result of rollbacks and 56 (30%) involved dangerous goods. The major outcomes of these occurrences were collisions (134, or 72%) and derailments (76, or 41%). Two of the occurrences (1%), including this occurrence, involved an employee fatality.
While switching without air is routine and occurs every day in the railway industry, the practice has some inherent risks that can result in serious consequences. If effective strategies are not taken to improve safety while switching without air, uncontrolled movements will continue to occur, increasing the risk and severity of adverse outcomes.
The railway industry is responsible for having rules, instructions, procedures, and processes in place to safely manage operations. Railway employees who are directly involved in these operations have the greatest knowledge of how the work actually gets done and are the most affected when accidents occur. However, the regulator also has a responsibility to have adequate regulations, rules, and enforcement in place in order to provide effective regulatory oversight to ensure safe operations.
Safety action taken by TC and the railway industry to date has focused on securement practices. However, the desired outcome of significantly reducing the number of uncontrolled movements has not yet been achieved.
The underlying causes of uncontrolled movements that occur while switching without air can vary greatly. Consequently, developing a comprehensive strategy to deal effectively with all of the underlying factors and associated risks in order to reduce the number of such uncontrolled movements is proving to be difficult. Therefore, the Board recommends that
The Department of Transport work with the railway industry and its labour representatives to identify the underlying causes of uncontrolled movements that occur while switching without air, and develop and implement strategies and/or regulatory requirements to reduce their frequency.
TSB Recommendation R20-01
1.0 Factual information
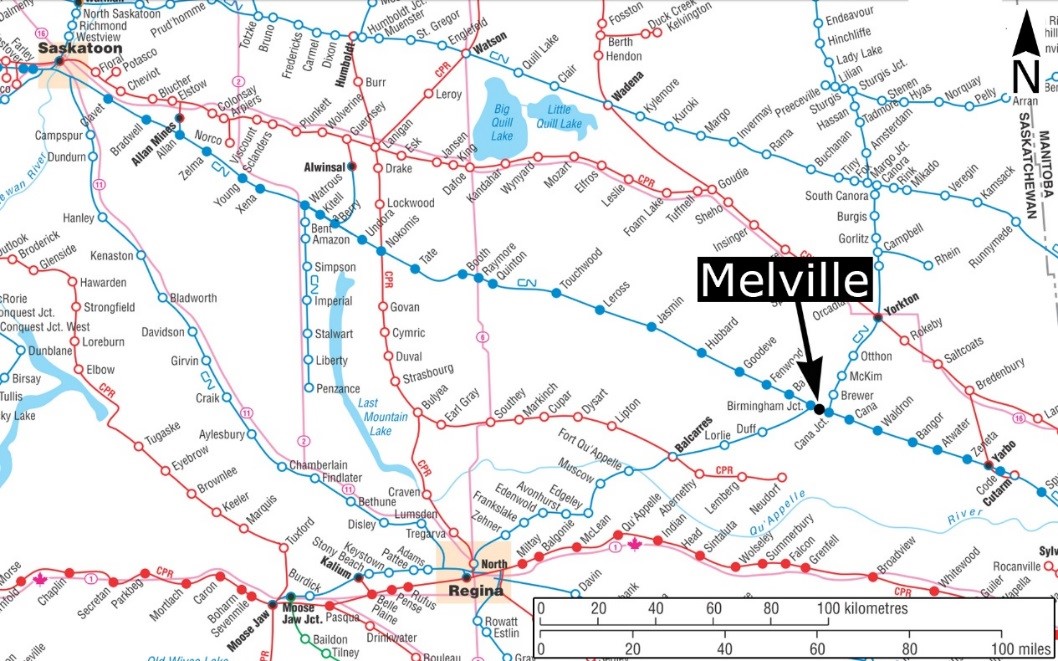
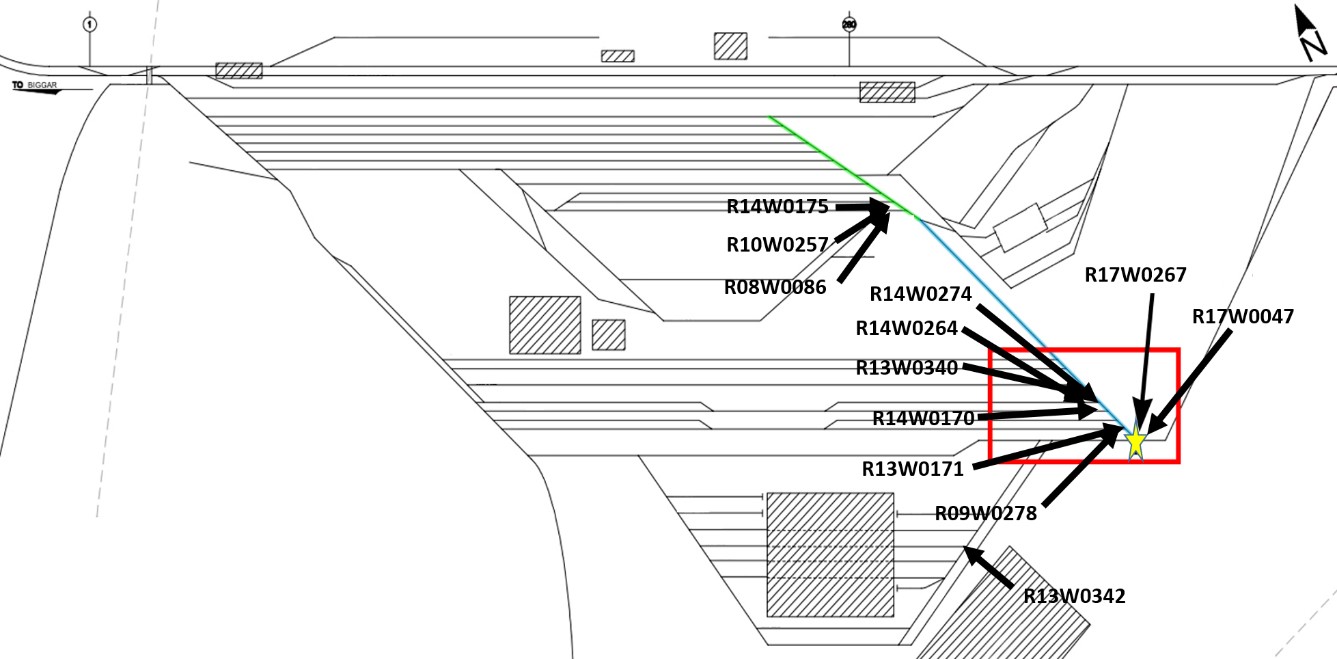
On 22 December 2017, Canadian National Railway Company (CN) extra yard assignment Y1XS-01 (the assignment), operated via a remote control locomotive system (RCLS), was performing switching operations at the east end of CN’s Melville Yard in Melville, Saskatchewan (Figure 1). The assignment consisted of 3 locomotives, 6 empty covered hopper cars,Footnote 3 and 3 open-top hopper cars loaded with ballast. The assignment was about 660 feet long and weighed about 1325 tons.
The crew consisted of 2 conductors, one acting as the yard foreman (foreman) in charge of coordinating the switching activities, and the other as the yard helper (helper). The crew members were qualified for their positions, met fitness and rest standards, and were familiar with Melville Yard. Both crew members wore green vests.Footnote 4 To perform the switching operations, each crew member was equipped with a remote control BeltpackFootnote 5 from which either crew member could operate the locomotive.
About 320 conductors and locomotive engineers (LEs) work out of Melville Yard. Work at Melville Yard consists of a combination of yard assignments, local switching assignments, and main-track freight trains.
At the time of the occurrence, there was a high volume of work and employees from other terminals had been transferred to Melville Yard to help with the increased traffic. Normally, 2 regular yard assignments worked daily. However, when the work could not be completed by the regular assignments and additional crews were available, extra yard assignments were called.
Yard work at Melville Yard was flat switching, primarily performed using RCLS. During switching operations, “kicking”Footnote 6 freight cars was a normal practice and was permitted throughout the yard. Access to the tracks from the east end of the yard was generally through the MR-lead track, which accessed tracks MR19 to MR10. The MR-lead track grade (east-to-west) ranged from 0.24% west of the MR19 switch to 0.50% between the MR16 and MR14 switches. The rest of the MR-lead track grade was generally undulating (Figure 2).
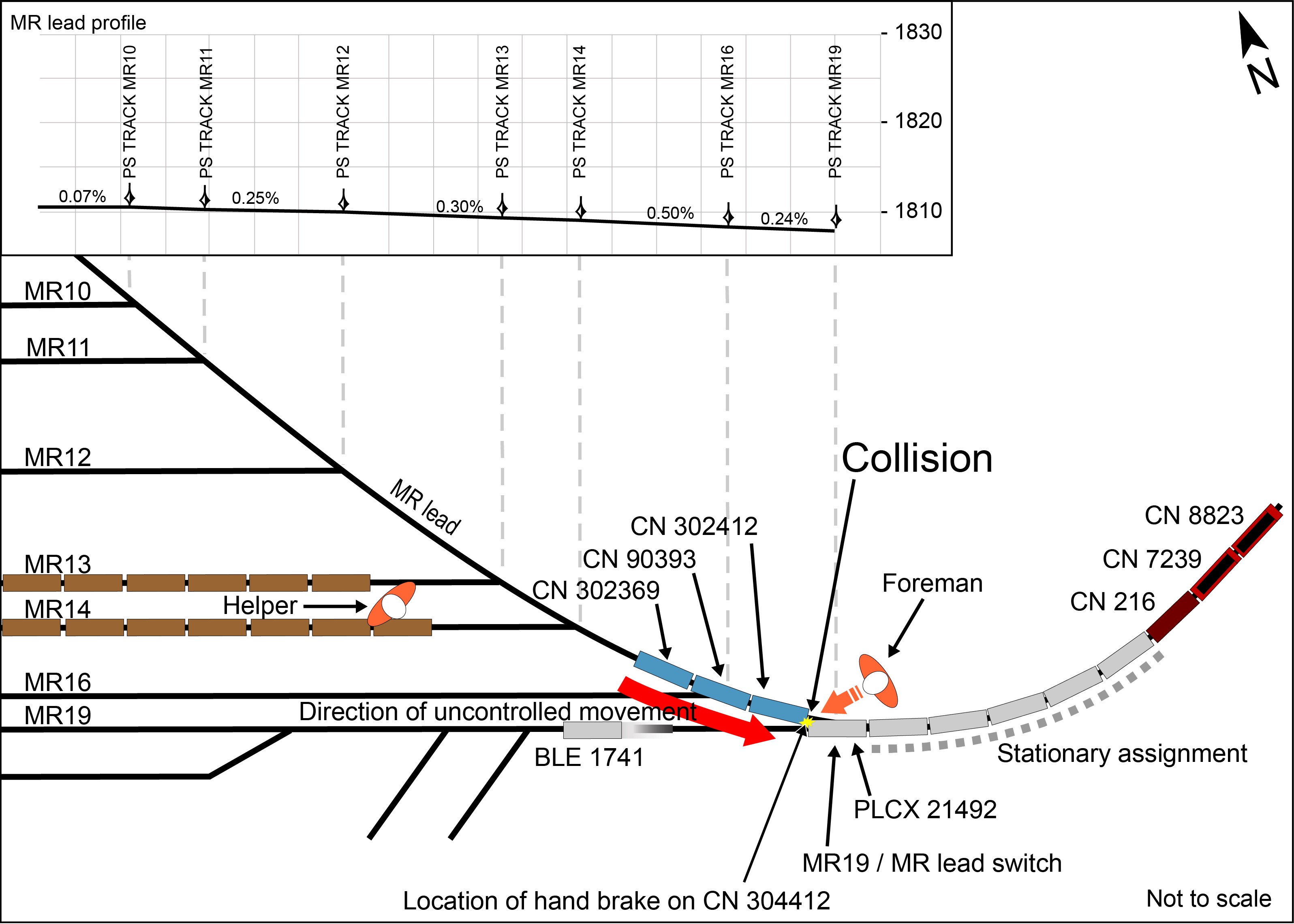
Note: “PS” means point of switch
1.1 The accident
At 1355,Footnote 7 the assignment crew members conducted a job briefing at the start of their shift. During the job briefing, the crew discussed the work to be performed during the evening by reviewing the switch lists that had been provided by the yardmaster. As was consistent with local practice, in addition to the crew’s normal duties (e.g., line switches, monitor the point of the movement, couple cars, and apply hand brakes), the foreman controlled all locomotive movements using the Beltpack.
Later in the shift, at about 1530, owing to mechanical problems with one of the switching locomotives, a high horsepower (HHP) road locomotive was added to the consist. Since the HHP locomotive had different performance characteristics compared to the switching locomotives, the trainmaster and assistant superintendent conducted a job briefing with the assignment crew to discuss the differences.
Upon completion of the job briefing, the crew members resumed their switching duties. The assignment travelled to the east end of the yard along the MR-lead track, pulling 10 cars. After it passed track MR13, the helper lined the switch for that track, and then walked to track MR19 to assist with setting off an empty covered hopper car (BLE 1741).
The foreman stopped the assignment just past the MR19 switch, lined the switch for track MR19, and then reversed the assignment into track MR19. When car BLE 1741 cleared the MR-lead track by about 200 feet, the helper contacted the foreman by radio and instructed her to stop the assignment. The helper applied the hand brake on BLE 1741, uncoupled the car, and left it in track MR19. The foreman then moved the assignment to the MR-lead track just east of the MR19 switch.
In preparation for placing the next 3 cars of the assignment into track MR13, the foreman lined the MR19 switch for the MR-lead track. In the meantime, the helper walked to cars that were already stationary in track MR13, about 50 feet from the fouling point of the MR-lead track. The helper assumed that the cars in track MR13 would have to be shoved westward to make room for the 3 open-top hopper cars loaded with ballast (CN 302369, CN 90393, and CN 302412) that were to be set off from the assignment.
The helper waited beside the stationary cars in track MR13, anticipating that the assignment would have to enter track MR13 to make a joint and push the stationary cars westward. From the helper’s position in track MR13, the eastward view of the MR-lead track was blocked by stationary cars in the adjacent track MR14. There was no communication between the crew members regarding the need to push stationary cars in track MR13 westward and the helper was unaware that the foreman intended to kick cars into track MR13.
After lining the MR19 switch, the foreman walked eastward along the north side of the assignment, past the 3 open-top hopper cars loaded with ballast, and lifted the uncoupling lever on the B end of CN 302412. She then placed the Beltpack speed selector to 7 mph and shoved westward before selecting “Stop” on the Beltpack.
As the assignment came to a stop, with the uncoupling lever on CN 302412 lifted, the 3 open-top hopper cars (Figure 3) released and separated (and thus were kicked) from the assignment. Under their own momentum, the 3 cars travelled on the MR-lead track over the MR19 switch toward track MR13. The remainder of the assignment stopped east of the MR19 switch.

After the 3 open-top hopper cars passed over the MR19 switch, the foreman lined the switch in preparation for setting off the remaining car in track MR19. As the assignment reversed into track MR19, she noticed that the 3 cars had begun to stall on the MR-lead track. The cars came to a stop with the leading B end of car CN 302412 almost parallel with the MR16 switch. After stopping, all 3 cars began to roll back toward the assignment.
Upon noticing that the cars were stalling, the foreman stopped the assignment with lead car PLCX 21492 partially in track MR19, but still foul of the MR-lead track (Figure 2).
The foreman then made a radio broadcast indicating that the 3 open-top hopper cars were rolling back. Hearing the radio broadcast, the helper, who was standing beside the lead car in track MR13, began to run toward the uncontrolled movement.
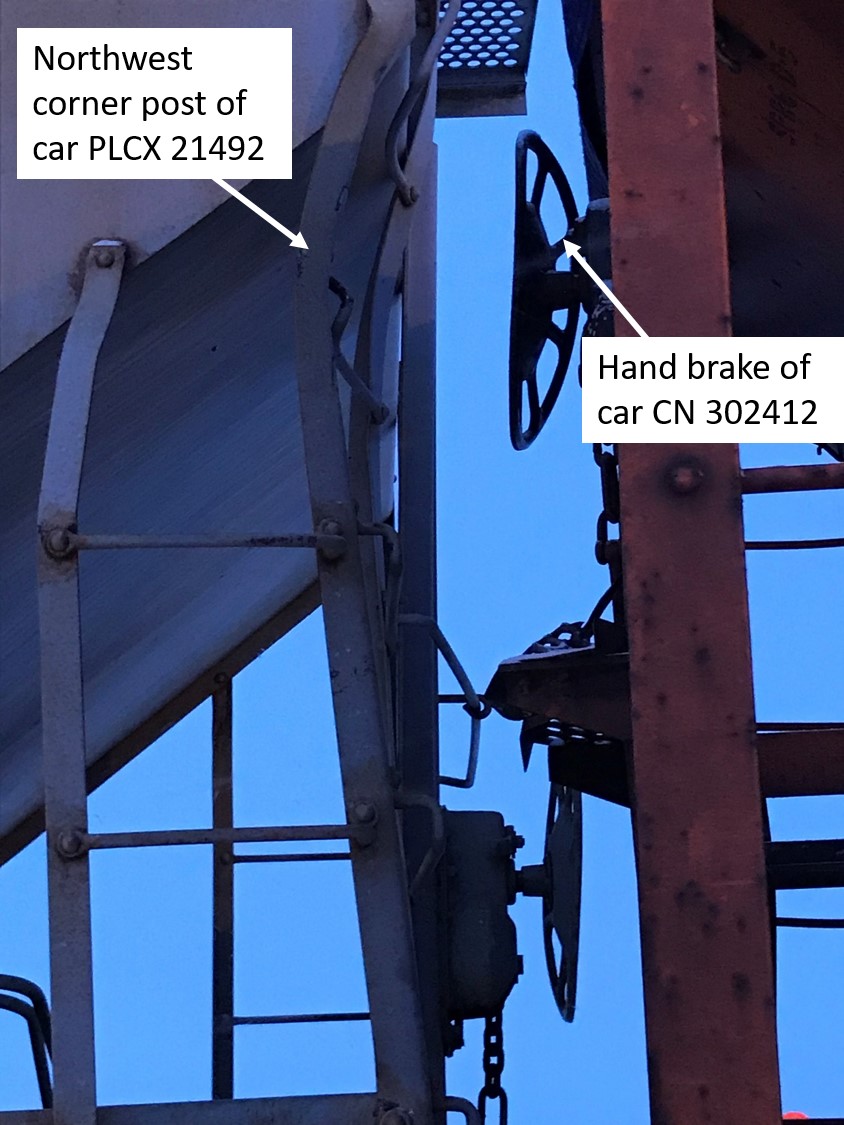
The foreman ran westward from the MR19 switch toward the leading B end of the lead car of the uncontrolled movement (CN 302412) in order to access the hand brake located near the top of the southeast corner of the car. The foreman reached the car and climbed the ladder that extended up to the CN 302412 B-end platform.
Once on the B-end platform, the foreman applied the high-mounted hand brake but could not stop the uncontrolled movement. Subsequently, the southeast corner of CN 302412 collided with the northwest corner of empty covered hopper car PLCX 21492, which was stationary and foul of the MR-lead track. The foreman became pinned between the corners of the cars (Figure 4) and received fatal injuries. There was no derailment and no dangerous goods were involved.
At the time of the occurrence, the temperatureFootnote 8 was −12.6 °C. Snow was falling and the wind was blowing at a speed of 22 km/h from the northwest.
1.2 Recorded information
The foreman had been kicking cars at 7 mph for most of the shift. Based on recorded information from the Beltpack and the locomotive event recorder, it was determined that:
- At 1801:35, the Beltpack was placed in the 7 mph position and the locomotives began to accelerate from a stop.
- At 1801:52, the assignment had reached 7 mph.
- At 1801:55, the Beltpack speed selector was reduced from 7 mph to Stop.
- At 1802:01, the assignment came to rest after having shoved about 155 feet westward in total.
- At 1802:44, the assignment had reached a speed of 4 mph.
- At 1802:57, an independent brake application was made.
- At 1803:04, the assignment came to a stop.
- At 1803:15, an emergency brake application occurred, 18 seconds after the independent brake was applied.
1.3 Hand brake application
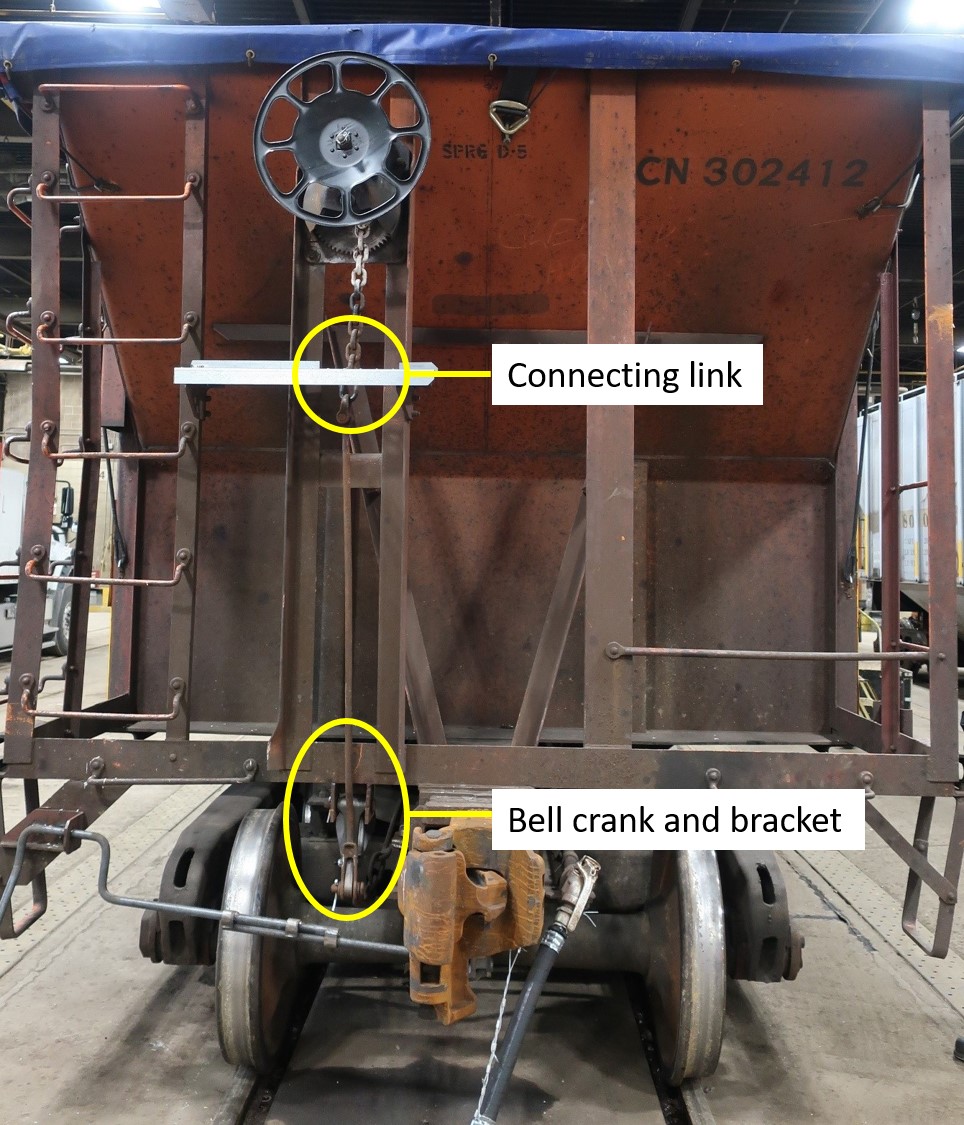
To apply the hand brake on a freight car, the wheel of the hand brake is turned clockwise, which draws the hand-brake chain into the hand-brake housing, applying tension to the connecting rod and the bell crank. The bell crank redirects the tension to the horizontal brake rigging attached to the brake cylinder, multiplying the tension at the brake shoes through a series of levers and rods.
The top portion of the hand-brake chain is painted white to help identify whether the hand brake is applied or not. Once the hand brake is applied, the white paint is no longer visible.
1.4 Post-accident examination of car CN 302412
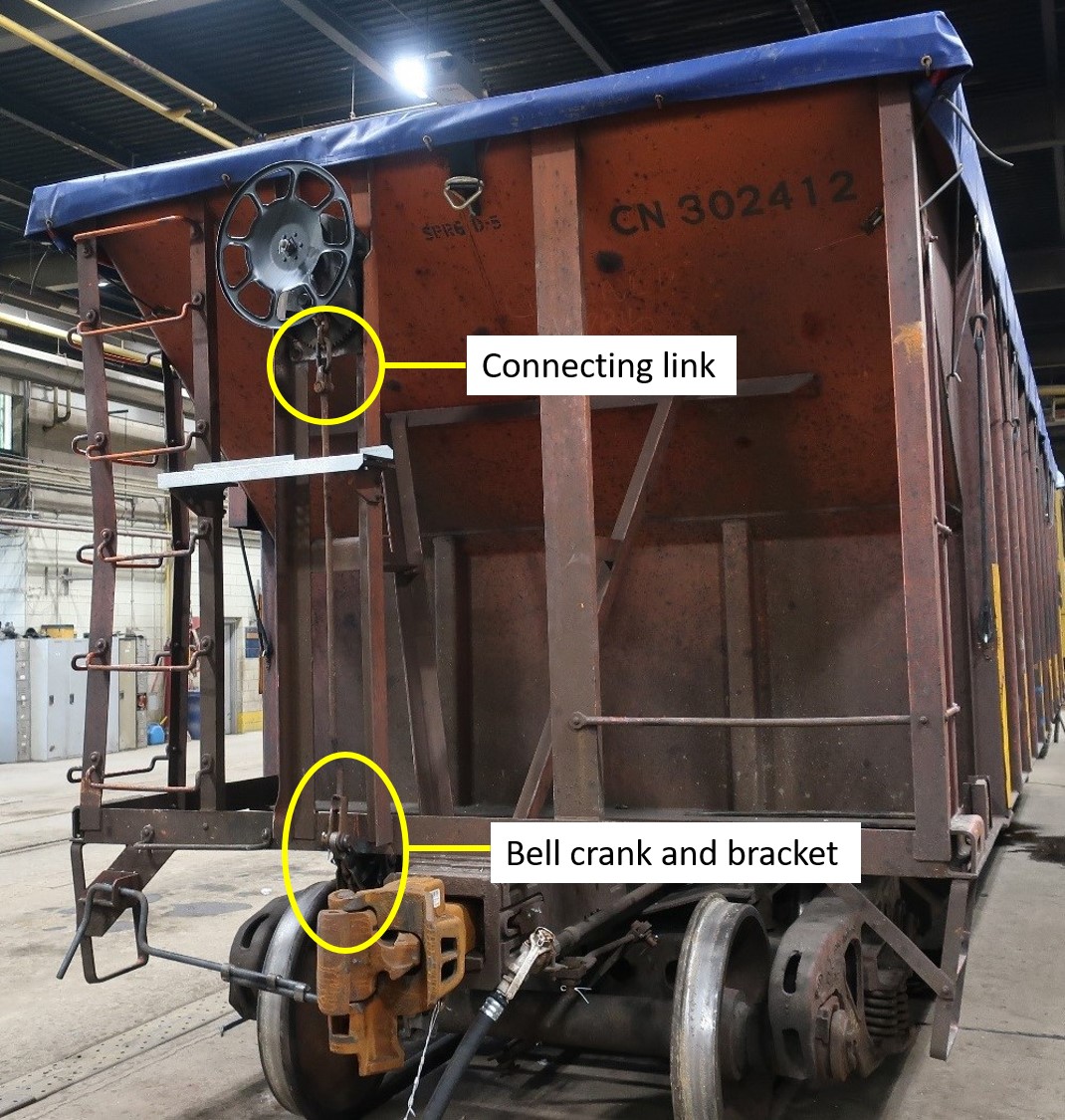
Car CN 302412 was a 70-ton, 44-foot-long open-top hopper car manufactured in 1974 by National Steel Car. The car weighed about 100 tons when loaded and was equipped with a hand brake that was mounted high up on the B end of the car. An elevated end platform was located about 90 inches from the ground, positioned below the hand brake.
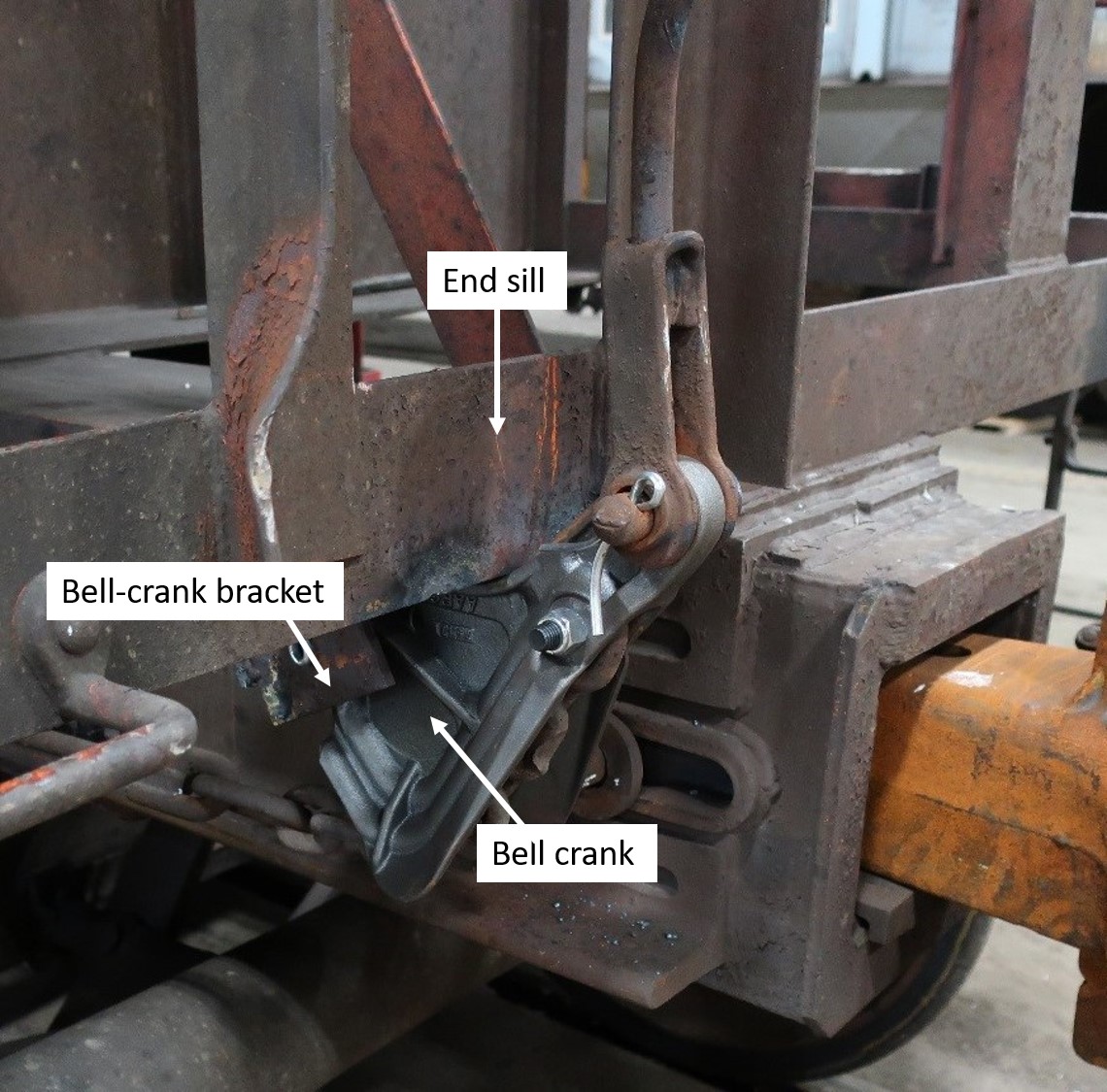
CN’s examination of car CN 302412 immediately following the accident determined that the hand brake chain, the connecting rod, and the bell crank were not in their proper positions. The large connecting chain link had pulled up close to the hand brake housing while the hand-brake connecting rod and the bell crank were pulled tight against the end sill (Figure 5). There was no white paint visible on the hand brake chain.

1.5 Accident re-enactment by the Canadian National Railway Company
On 23 December 2017, CN conducted an accident re-enactment in Melville Yard. The re-enactment simulated the moves performed by the assignment crew, including attempting to kick the same 3 open-top hopper cars loaded with ballast from the MR-lead track into track MR13. The re-enactment determined that:
- Similar to the actual occurrence, the 3 open-top hopper cars did not make it into track MR13. Instead, they stopped and rolled back.
- With the CN 302412 hand brake and rigging unaltered from the day of the accident, the hand brake was again applied but could not hold the same 3 cars.
The 2 cars involved in the collision (PLCS 21492 and CN 302412) were photo-documented and examined more closely, which included documenting the broken bell-crank bracket (Figure 6).
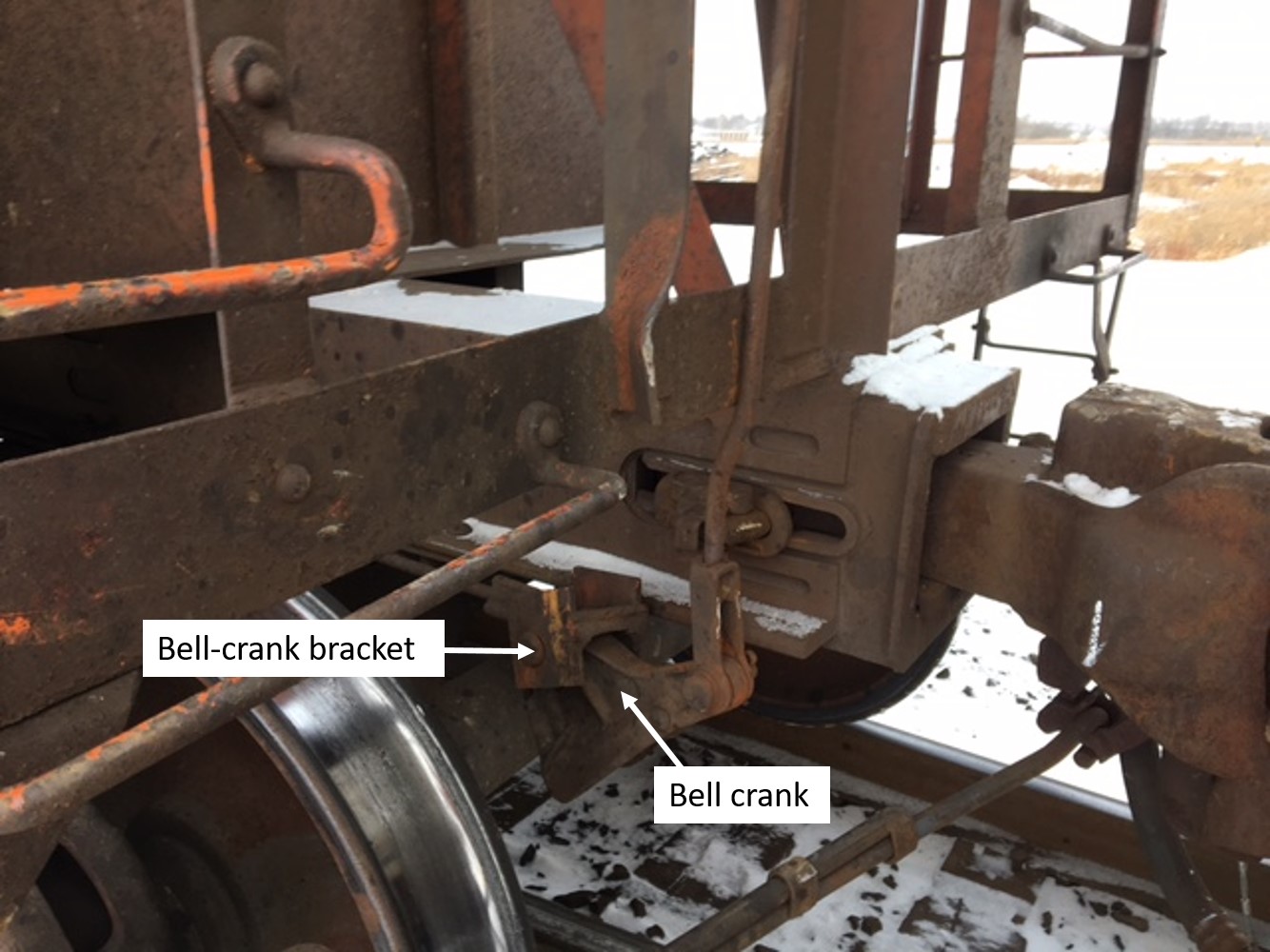
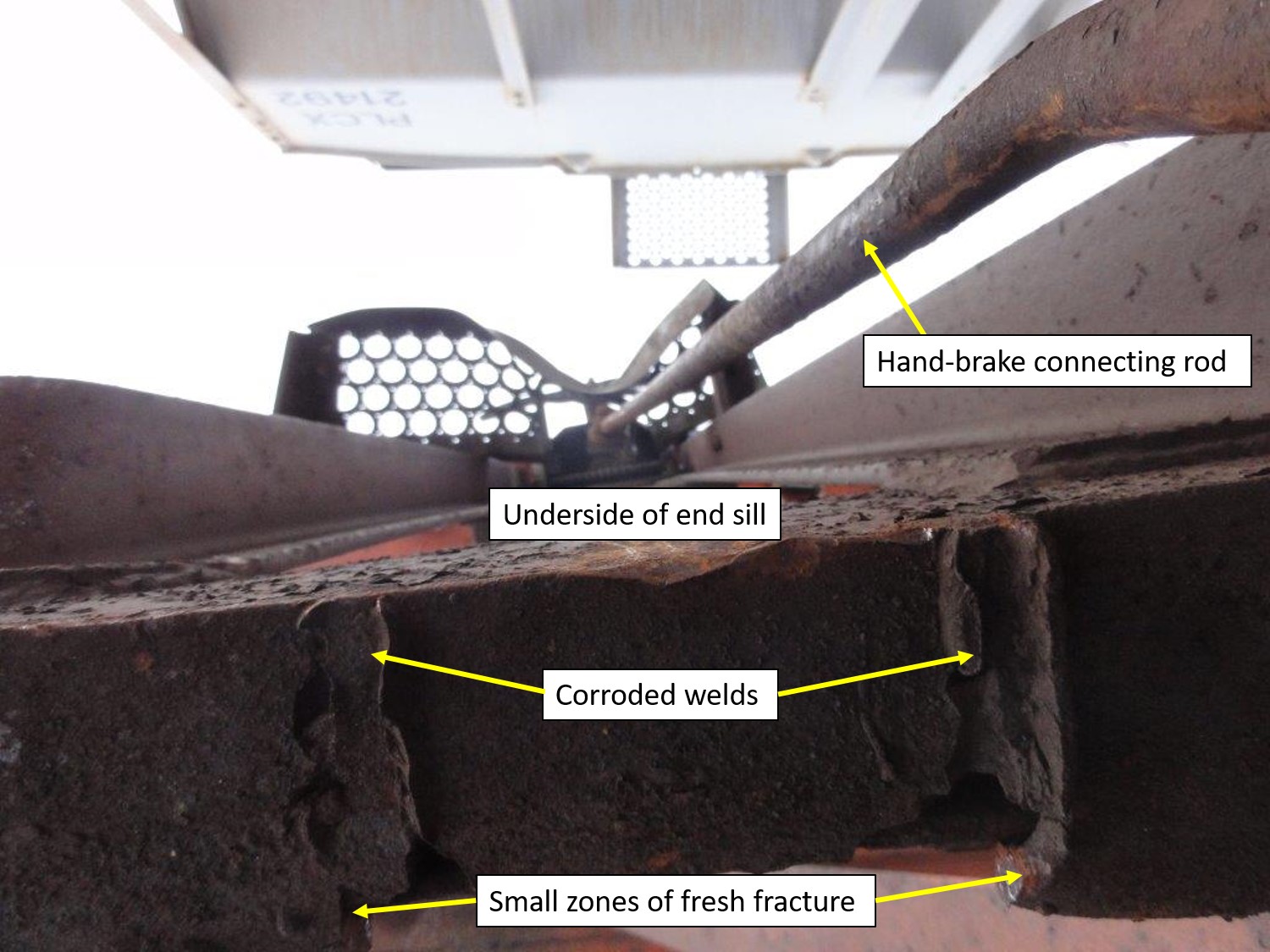
Examination of the bell-crank bracket and the bell crank determined that the welds securing the bell-crank bracket to the underside of the CN 302412 B-end sill had failed, and the bracket fracture surface contained 2 small zones of fresh fracture (Figure 7).

The fracture surfaces of the welds displayed heavy corrosion. The extent of the corrosion suggests that it had been present for an extended period of time. The rear of the 2 outboard welds each contained a small bright area, which was consistent with the 2 small zones of fresh fracture observed on the bell-crank bracket fracture surface (Figure 8).
Following the accident re-enactment, CN 302412 was sent for repairs, which included welding the bell-crank bracket back onto the end sill, installing a new bell crank, installing a new end platform, repairing various brake rigging components, and conducting a full single-car air-brake test while on a shop track. The hand brake wheel was replaced, but the hand brake itself did not require repair and remained with the car. After verifying that the car was safe to travel, it was sent to CN’s Symington Yard car shop in Winnipeg, Manitoba.
1.6 On-site re-enactment by the TSB
During the week of 15 January 2018, the TSB conducted additional re-enactments in Melville Yard using 3 similar open-top hopper cars loaded with ballast. The 3 cars were kicked at various speeds from the same location as the occurrence cars. It was determined that:
- When the 3 cars were kicked at 7 mph, the cars stalled and came to rest with the leading B end of the 3rd car in the vicinity of the MR16 switch about 50 feet away, before rolling back.
- With no hand brake applied, it took 22 to 30 seconds for the cars to travel to the point of impact after they began to roll back.
- When the 3 cars were kicked at 10 mph, the cars successfully rolled into track MR13 and did not roll back.
The assignment and cars were staged and secured at the approximate locations of the foreman and the uncontrolled movement cars just prior to the accident. On average, it took about 18 seconds for a person to react and run from the north side of the MR19 switch (i.e., where the foreman was positioned) to the approximate location of car CN 302412, climb the ladder to access the hand-brake end platform and fully apply the hand brake. Based on the TSB re-enactment, CN 302412 likely stalled and came to rest with the leading B end in the vicinity of the MR16 switch, about 50 feet away.
Because it took 22 to 30 seconds for the cars to travel to the point of impact after they began to roll back, and it is not known precisely when the foreman began to run toward the cars, it is possible that the foreman might have had more than 18 seconds to apply the hand brake.
1.7 Hand-brake force testing of CN 302412
On 25 January 2018, the TSB conducted hand-brake force testing on open-top hopper car CN 302412 at the Symington Yard car shop. In preparation for testing, the car was placed inside the car shop with no hand brake applied (Figure 9).
During testing, the hand brake (which had been repaired) was fully applied (Figure 10). The position of the hand brake components was recorded.

With the hand brake fully applied, the positions of the repaired hand brake components were compared to the position of the components following the accident, but before repairs (Figure 5). Before repairs, the large connecting chain link had pulled up close to the hand brake housing rather than remaining below the housing. In addition, the hand-brake connecting rod and bell crank were pulled tight against the end sill.
1.7.1 Brake-shoe force testing
According to the Association of American Railroads (AAR) Manual of Standards and Recommended Practices (MSRP) Standard S-401, Brake Design Requirements, a freight car hand brake is required to generate a net braking ratio (NBR) of 10% with a chain force of 3350 pounds at the time of manufacture.Footnote 9 The hand brake NBR is determined by dividing the sum of the hand brake force at each wheel, for a fully applied hand brake, by the gross rail load of a fully loaded car. The minimum allowable NBR for a car in service is 6.5% with a hand brake application of 125 foot-pounds of torque.Footnote 10
For car CN 302412, brake shoe force tests were conducted to ensure that the hand brake itself was functioning properly. The hand brake was applied using a torque wrench and the brake shoe force was recorded at torque values of 25, 50, 75, 100, and 125 foot-pounds, respectively. The brake shoe force was measured at each of the freight car wheels. The NBR for the CN 302412 hand brake, with the bell-crank bracket properly attached and a torque application of 125 foot-pounds, was calculated to be 8.89%, which exceeded the AAR minimum requirement, indicating that the hand brake functioned as intended.
After cutting the bell-crank bracket from the B-end sill to simulate a broken condition, subsequent testing was conducted. The same brake shoe force tests were performed with the bell-crank bracket and the bell crank separated from the car body. When the hand brake was applied, these 2 components moved into almost the identical positions in which they were found at the accident site (Figures 11, 12, and 13). The highest NBR achieved for this test was 2.42%, which did not meet the minimum required NBR of 6.5%. This indicates that a hand brake with rigging in this condition is ineffective.

1.7.2 Stopping distance calculations
The investigation sought to understand the effect that a fully functioning hand brake could have had on the stopping distance of the 3 loaded cars in this occurrence. Stopping distance was calculated based on the force of gravity, the rolling resistance of the cars, the rate of acceleration, and the hand brake force of an uncompromised hand brake.
Based on the TSB on-site re-enactment, when the cars started to roll back, during the 18 seconds that it took a person to react and fully set the hand brake, the cars would have reached a speed of about 1.72 mph and travelled a distance of 22.7 feet. This calculation assumes that the hand brake would have been completely ineffective until it was fully applied.
If the hand brake had been fully applied using 125 foot-pounds of torque and had been fully effective, the 3 cars would have come to a stop within an additional 21.2 feet.
1.8 Regulatory requirements for hand brake positioning
Train operations have changed over the years and there is no longer a need to have hand brakes positioned near the top of a car. As a result, many older cars have been modified by lowering the hand-brake end platform, positioning it nearer to the bottom of the car body.
Rail cars built after 01 January 2015 are required to be manufactured with the hand-brake end platform (brake step) located no more than 8 inches above the centre sill, which is about 48 inches above the top of the rail. Footnote 11,Footnote 12
1.8.1 Transport Canada Railway Freight Car Inspection & Safety Rules
The Transport Canada (TC)–approved Railway Freight Car Inspection & Safety Rules prescribe the minimum safety standards for freight cars operated by railway companies pursuant to the Railway Safety Act. Part III of the rules, “Other Requirements,” states:
17. Design
- 17.1 Every new freight car shall be designed and constructed in accordance with the “Association of American Railroads Manual of Standards and Recommended Practices”, or to an equivalent standard to provide for safe operation.
- 17.2 Every new freight car built after January 1, 2015 shall be designed and constructed with safety appliances in compliance with the latest edition of AAR Safety Standard S-2044 “Safety Appliance Requirements for Freight Cars” of the Manual of Standards and Recommended Practices. Cars built prior to January 1, 2015 shall be designed and constructed with safety appliances in compliance with General Order No. 0-10, “Regulations Respecting Railway Safety Appliance Standards”.Footnote 13
1.8.2 U.S. Federal Railroad Administration Code of Federal Regulations
The Federal Railroad Administration (FRA) Code of Federal Regulations section 231.2, titled Hopper cars and high-side gondolas with fixed ends, item (a) (3) (i), states that:
Each hand brake shall be so located that it can safely be operated while car is in motion.Footnote 14
1.8.3 Association of American Railroads Manual of Standards and Recommended Practices
Standard S-2044 in the AAR MSRP establishes requirements for safety appliance arrangements applied to railway cars built new on or after the mandatory dates specified for each car type. Specifications for open-top hopper cars, used for hauling ballast, are defined in Appendix F1. According to section 2.2.1 of Appendix F1, the location of the hand brake wheel is required to be no less than 28 inches and no more than 40 inches above the end platform.
2.2.1 The hand brake shall be located so that it can be safely operated from the horizontal end platform while the car is in motion. The center of the hand brake shaft on cars equipped with one hand brake shall be located on the B end of the car to the left of, and not less than 17 in. nor more than 22 in. from, the centerline of the car and shall be not less than 28 in. nor more than 40 in. above the platform-support surface of the end-platform mounting brackets. The hand brakes on cars equipped with more than one hand brake shall be located as specified in paragraph 9.0 of the base standard.Footnote 15 [emphasis in original]
S-2044 was approved by the AAR and the FRA. While S-2044 does not permit high-mounted hand brakes on any car types, it does not require high-mounted hand brakes to be re-positioned on cars built prior to the date that S-2044 became effective for that car type.
1.9 Safety appliances on railway cars
Section 4.2 of Standard S-2044 states that safety appliances must be securely fastened to a car, meaning that they are “[a]pplied with two-piece rivets, with one-piece rivets, or with threaded bolts.”Footnote 16
Section 5.8 of the standard states:
The portions of the hand brake system that are considered safety appliances, and are therefore required to be securely fastened as defined in paragraph 4.2, are the hand brake housings and hand brake operating levers. Unless otherwise specified in individual appendices to this standard, hand brake mounting brackets shall be securely fastened. Bell crank mounting brackets, sheave wheel mounting brackets, brake rod supports and guides, and chain supports and guides are not considered safety appliances. They need not necessarily be securely fastened and may be applied by welding. [emphasis in original]Footnote 17
1.10 Freight car inspection and maintenance
Part I (General), section 4 (Safety Inspections) of the Railway Freight Car Inspection & Safety Rules requires a railway company to ensure that freight cars it places or keeps in service are free from all safety defects described in Part II of the Rules. Specifically, it states that:
4.1 Subject to sections 20 and 21, of these Rules, a railway company shall ensure the freight cars it places or continues in service are free from all safety defects described in Part II of these Rules, and that such cars comply with General Order No. 0-10, “Regulations Respecting Railway Safety Appliance Standards”, or the latest edition of AAR Safety Standard S-2044 “Safety Appliance Requirements for Freight Cars” of the Manual of Standards and Recommended Practices.
4.2 Safety inspections shall be performed by certified car inspector(s) at safety inspection locations
- where trains are made up;
- on cars added to trains;
- where cars are interchanged. […] Footnote 18
The Railway Safety Appliance Standards RegulationsFootnote 19 require that safety appliances be secured to a car body using ½-inch bolts or rivets. Consequently, welding is not permitted.
When inspecting safety appliances, certified car inspectors at CN are taught (as part of the CN Car Inspection Train Yard course) to check that the safety appliances are in place, properly secured, in good condition, and meet the required clearances.
When inspecting the hand brake, certified car inspectors at CN are taught to ensure the following:
- There is adequate clearance for the operator’s hand (minimum 4 inches).
- The brake chain is attached to the hand brake and to the rod.
- The hand brake is in the fully released position.
They are also instructed to check that the hand brake and the bell crank are in good condition. If either appears damaged, the certified car inspector is to further check that the hand brake is operational.
The Railway Freight Car Inspection & Safety Rules require an inspection of the train or the cars added to the train before departure. Appendix 1, Pre-Departure Inspection, requires the inspection to include:
- car body related hazards:
- car body leaning or listing to the side;
- car body sagging downward;
- car body positioned improperly on the truck;
- object dragging below the car body;
- object extending from the side of the car body;
- door insecurely attached;
- broken or missing safety appliance; and
- lading leaking from a placarded dangerous goods car;
- overheated wheel;
- broken or cracked wheel;
- hand brake that failed to release; and
- any other apparent safety hazard likely to cause an accident or casualty before the train arrives at its destination.Footnote 20
In addition to inspection requirements when cars are part of a train, Item E.4 from Rule 13 of the Field Manual of the AAR Interchange Rules states that geared hand brake mechanisms and connections must be inspected, tested, and lubricated when a car is on a shop track or a repair track.Footnote 21 Hand brakes must also be inspected during the single-car air-brake test,Footnote 22 which requires the inspector to observe that the bell crank is in the normal working range.Footnote 23 However, there is no specific requirement to inspect the welds that secure a bell-crank bracket to the end sill of a car. Air brake equipment is addressed by Rule 7 of the Field Manual of the AAR Interchange Rules (Brake Beams Hangers, Brackets, Wear Plates and Brake Connection Pins, Hanger Pins or Bolts). Section A – Wear Limits, Gaging, Cause For Renewal indicates that during inspection, worn connection pins or bolts must be renewed when the original diameter exceeds measurements by 1/8 inch or more. However, there are no specific requirements for inspecting welds.
In the 10 years preceding the accident, car CN 302412 had been on a shop or repair track 23 times for repair. On 5 of these occasions, a single-car air-brake test was conducted. The most recent single-car air-brake test performed on the car was in July 2013 at Symington Yard in Winnipeg. The due date for the next air-brake test stencilled on the car was 28 December 2019. The most recent certified car inspection for the car was performed at Symington Yard on 19 December 2017 (3 days before the occurrence), with no defects noted. The car departed the following day on a westbound freight and was set off in Melville.
1.11 Canadian National Railway Company’s ballast car fleet inspections
Following the occurrence, CN identified 857 similar open-top hopper cars built by National Steel Car and of a similar age. CN immediately began to remove these cars from service in order to inspect them for similar conditions (i.e., with the hand brake and related brake rigging components). The work on each car included a single-car air-brake test and a full inspection of the hand brake and all brake rigging to ensure safe operation.
At May 2019, all 857 cars had been inspected. The inspections identified 63 cars with a cumulative total of 71 defects. Of the 71 defects, 52 could potentially affect the safe operation of hand brakes (Table 1).
| Location of defect | Number of defects |
|---|---|
| Brake step | 10 |
| Hand brake | 15 |
| Bell-crank bracket | 5 |
| Ladder bracket | 2 |
| Bottom rod | 1 |
| Bottom rod support | 16 |
| Brake pin | 3 |
| Total | 52 |
1.12 Crew information
In the rail industry, conductor positions are generally unionized positions governed by collective agreements between the employer and the employee union. At CN’s Melville Yard, local assignments are posted for bidding each week. After the employees submit their bids, the positions are awarded based on seniority in accordance with the collective agreement. Some of the posted positions are favoured owing to the rate of pay, days off, and hours of work. Typically, the evening shifts and the night shifts are considered the least desirable. In addition, yard positions are normally regarded as the least desirable because the pay rates for these positions are the lowest.
If no job bids are received for a specific position, the position is typically awarded to the employee with the least seniority, in accordance with the collective agreement. As there has been extensive employee turnover in the rail industry in the past few years, it is not unusual for the 2 most junior and least experienced employees at a terminal to be working together in yards, particularly during the evening and night shifts. The pairing of inexperienced crew members is not uncommon in the Canadian rail industry.
However, CN has measures to support a crew of 2 newly qualified employees who are working together. For example, green vests are used to identify employees with less than 2 years of experience, which helps promote coaching and mentoring from more experienced employees, on-the-job trainers, and management. When newly qualified employees are working together, frontline supervisors are encouraged to participate in the job briefing when possible. In this occurrence, the assignment was an extra yard assignment. This meant that the crew had been called from the spareboard (a list of employees on call or on standby) by identifying the next 2 RCLS-qualified employees. The employee with the most seniority was designated to act as the foreman.
Colleagues, instructors, and managers described both crew members as being competent, conscientious, and quick to learn. However, both crew members were also described as having a tendency to be reserved.
The occurrence crew had only worked together on 1 other occasion in October 2017.
1.12.1 Foreman
The foreman began conductor training in September 2014 and qualified as a conductor in February 2015, after completing classroom training and working on 37 freight train trips and 14 yard shifts. In November 2015, the foreman attended a 2-week RCLS training course at Melville Yard and became qualified as an RCLS operator.
In April 2016, the foreman was laid off from CN. Between April 2016 and March 2017, she was employed as a conductor at Cando Rail Services to switch rail cars at the Mosaic Company potash mine in Esterhazy, Saskatchewan. During that time, she worked as a conductor and was part of a 3-person crew that included an LE. No RCLS-controlled switching was performed at the potash mine. While employed by Cando Rail Services, the foreman attended 2 quarterly safety meetings and underwent 14 proficiency tests. Of the 14 proficiency tests, 13 were compliant, but 1 test identified an at-risk behaviour related to the need for 3-point protection during train operations. There was no record of any discipline.
In March 2017, the foreman returned to work full time at CN. Since returning, the foreman had worked primarily on the road, but did work 22 shifts at Melville Yard: 5 shifts as a foreman, and 17 shifts as a helper. During that time, the foreman underwent CN proficiency testing on 4 occasions, during which 15 observations were made and no at-risk behaviours were noted.
A sleep-wake history of the foreman was not available, and so a detailed fatigue analysis could not be carried out. However, the time of day when the occurrence took place and the foreman’s work schedule were not indicative of the potential for fatigue, and fatigue was not considered to have played a role in this occurrence.
1.12.1.1 Previous accident involving foreman
On 21 October 2017, the foreman (while acting as a helper) was involved in a derailment in Melville Yard.Footnote 24 In that occurrence, the front 3 axles of the lead locomotive of the crew’s yard assignment derailed. The railway’s internal investigation attributed the derailment to an improperly lined switch. As the foreman had no at-risk behaviour incidents during the previous 12 months, the corrective action consisted of mentoring and coaching rather than disciplinary action.
1.12.2 Helper
The helper began conductor training in February 2017, and qualified as a conductor in June 2017 after completing classroom training, 41 freight train trips, and 17 yard shifts. In August 2017, the helper attended a 2-week RCLS training course at Melville Yard and became qualified as an RCLS operator.
While working at CN, the helper had no history of disciplinary action and had been proficiency tested 5 times, with 15 observations made and no at-risk behaviours noted.
The helper was one of the employees with the least seniority at the Melville terminal. As such, the helper was often assigned to a position in the yard. Since qualifying as an RCLS operator, the helper had worked 40 shifts in Melville Yard, including the accident shift. Of the 40 shifts, the helper worked 37 shifts acting as the foreman paired with a more junior employee acting as a helper.
1.13 Kicking cars
When kicking cars during switching operations, judgment is required to choose the speed and location at which to release the cars to ensure that the cars have sufficient momentum to roll into the intended track. The operator must also ensure that the momentum of the cars does not cause them to couple to equipment already in the track at an excessive speed.
CN’s General Operating Instructions (GOI) stipulate that “speed must be regulated to ensure that coupling speed does not exceed 4 MPH.”Footnote 25 Learning to do this requires practice to develop the required judgment because there are multiple variables involved, including the number of cars, the weight of the cars, the presence of a grade, and the environmental conditions. The GOI also state that a kicked car must not be allowed to roll back and foul other tracks or contact other pieces of equipment.Footnote 26
CN’s RCLS operator training video states that “setting the right speed is the trickiest part” when kicking cars during RCLS operations. With no readout of actual speed on the Beltpack, the operator is required to make this judgment on the speed and location at which to release the cars based on an estimation of the speed.
During RCLS training at Melville Yard, conductor trainees were told that the speed selector should be set to 10 mph before accelerating the locomotives. The trainers also emphasized that, when kicking cars in Melville Yard from the MR-lead track into tracks MR19 to MR10, the ascending track gradient in the area could be problematic. In these cases, the guidance was to have a crew member in a position to be able to observe the cars and intervene by boarding the cars and applying hand brakes if the cars began to roll back unexpectedly.
At Melville Yard, crews were also instructed to make a radio broadcast just before kicking cars, stating the number of cars that were being kicked and the name of the track they were being kicked into. The radio broadcast was intended to keep all crew members informed. This is a local practice rather than a CN system requirement. In this occurrence, there was no indication that the foreman had broadcast over the radio that the cars were being kicked into track MR13.
1.14 Requirements to conduct job briefings
The purpose of a job briefing is to ensure that all work is understood between crew members. CN’s GOI establish the requirements for crews to conduct job briefings.
Section 8 – Safe Work Procedures of the GOI establishes responsibility for safety. Specifically, Item 3.1 (e) states:
Perform job briefings to ensure understanding of the work to be done including evacuation procedures, first aid, hazard identification, safety procedures, and the communication needed to protect all people working on the job.Footnote 27
The GOI provide additional details on job briefings “to ensure crew members communicate critical information pertaining to safe train operations prior to and throughout their tour of duty.”Footnote 28 This procedure specifies that a job briefing should include a discussion of the sequence of basic job steps, as well as the potential hazards and how to protect against them. The procedure also specifies that employee responsibilities should be confirmed and additional job briefings must be held when work conditions change.
Examples of working conditions to be discussed during the job briefing include
Track characteristics (grade and curvature), weather conditions (i.e. wind), type of equipment (i.e. partially loaded tank cars may move due to sloshing action, bulkhead flats and wind) […] .Footnote 29
At Melville Yard, yard crew members were expected to conduct job briefings before their shift and when conditions changed, and to communicate switching moves over the radio to keep everyone informed.
1.15 Previous uncontrolled movements at Melville Yard
A review of the TSB Railway Occurrence Database System (RODS) for uncontrolled movements at Melville Yard from 2008 to 2017 revealed 11 previous uncontrolled movements (Appendix A). Of the 12 uncontrolled movements, including this occurrence, 8 had occurred along the MR-lead track between the MR13 and MR19 switches (Figure 14).
Of the 11 previous occurrences, the most recent occurred on 26 February 2017 at the same location as the occurrence under investigation. At that time, the cars were being switched between track MR19 and the MR-lead track.
CN indicated that most of the previous uncontrolled–movement incidents in that area of the yard involved inadequate securement and operator errors. Corrective measures focused on employee education, clarification of instructions to the employee, increased employee monitoring, and disciplinary action (in some cases).
During the investigation, it was determined that rollbacksFootnote 30 were common on the MR-lead track and that many employees had experienced rollbacks. However, railway employees are unlikely to report events that do not result in an adverse consequence to the railway company, because they could potentially be subject to disciplinary action by the company. Therefore, the total number of uncontrolled movements in Melville Yard (including rollbacks, and those movements that did not result in damage) was likely higher than the occurrences identified in RODS.
If employees are encouraged to report close calls (such as rollbacks that do not result in an adverse consequence) without fear of discipline, railways can identify hazards and take mitigating actions before an accident occurs.
1.16 Remote control locomotive system
The RCLS consists of 3 components:
- one or more remotely controlled locomotive(s) (RCLS-controlled locomotive);
- an on-board control computer, which is mounted inside the RCLS-controlled locomotive to interface with the controls; and
- an operator control unit (OCU), commonly referred to as a Beltpack (Figure 15).
The Beltpack is a lightweight remote-control device that attaches to the operator’s safety vest (Figure 16) and controls the RCLS-controlled locomotive.


Yard crews work in teams of 2. The crew members can pass control of the locomotive(s) back and forth as required (which is referred to as “pitch and catch”) but only 1 crew member has control at a time. The Beltpack is equipped with a speed selector that has 8 settings, including pre-adjusted speeds of 4 mph, 7 mph, 10 mph, and maximum speed (15 mph); a forward and reverse selector; and a brake selector that includes an emergency brake feature. The Beltpack does not display the actual speed of the locomotive.
Once a speed is selected, the Beltpack applies either the throttle or the brakes of the locomotive(s) to attain the pre-selected speed, then maintains the selected speed to within ± 0.5 mph.
1.17 Federal Railroad Administration report on the safety of remote control locomotive operations
In 2002, to better understand the safety implications of RCLS operations, the FRA initiated a multi-study research program. In March 2006, the FRA published Final Report: Safety of Remote Control Locomotive (RCL) Operations. Although the study was primarily focused on the practices of U.S. railroads, one of the focus groups included Canadian railways.Footnote 31 The report analysis and results were applicable to the North American railway industry.
The report addressed human factors issues, including remote control operator training, preparation, and experience. On this subject, the report stated that
[t]he combination of increase in new hires with no prior railroad experience (especially switching experience) and self-reported and observed (via Foster-Miller research) inadequacies in RCO [remote control operator] training and preparation have the potential to be problematic and may lead to RCO errors, as well as accidents/incidents due to a lack of knowledge or understanding of RCL operations, including switching operations.Footnote 32
Examples of inadequacies in the training included:
- Insufficient or poor-quality training on a specific move to be made or a specific area of a yard
- Inadequate on-the-job training
- Insufficient amount of hands-on training
The report also expressed concerns about the large influx of new workers into the railways. It noted that the abundant experience that the current locomotive remote control operators had when they were learning to operate RCLS was extremely important in maintaining a safe working environment. The FRA expressed concern that the current workers learning RCLS operations would not be afforded the traditional breaking-in periods when learning their jobs, especially RCLS jobs.Footnote 33
Among others, the report identified the pairing of inexperienced crew members as a critical safety issue. Given the industry shortage of switchmen and LEs, it was thought that this may be a significant safety issue in the future.Footnote 34
In the past, many of the employees who were initially trained in the use of RCLS technology had significant railway experience to draw on. Experienced employees were familiar with railroad safety, operating rules, and the intricacies of working in busy classification yards.Footnote 35
1.18 Training and qualification of railway operating employees
New CN operating employees must first qualify as conductors. At CN, the conductor training, which can last about 6.5 months, consisted of the following components:
- 7-week orientation and rules training;
- up to 2 weeks of “boot camp” field training in a controlled setting; and
- a mandatory minimum of 45 trips under the guidance of a qualified conductor, which takes about 4.5 months.
On completion, new employees were considered qualified to act as yard helper, conductor, or yard foreman.
After qualifying as a conductor, and as required by the railway based on operational needs, new conductors at Melville Yard received their RCLS training. This training consisted of a 1-week classroom component and a 1-week practical component under the supervision of a local instructor. Classes were usually made up of 4 trainees.
During the week of practical training, the trainees occupied a dedicated section of the yard where they would practice switching in a controlled environment. The trainers tried to ensure that each trainee had at least 8 hours operating the RCLS-controlled locomotive during the practical training. To qualify as an RCLSoperator, employees were required to demonstrate certain key skills, such as coupling and kicking cars. Additional practical training was allotted if employees were unable to demonstrate that they were proficient at the key skills.
Section 6 of CN’s GOI contains instructions for RCLS operations. Section 6.5.1 states that “[t]he employee on the point of [the] movement should be in control of critical stop movements when practicable.”Footnote 36
At Melville Yard, the RCLS training included procedures for coordinating movements between 2 RCLS operators through the pitch-and-catch feature on the Beltpack to ensure that the operator controlling the movement is in a position to observe the point of the movement. However, it was common practice at Melville Yard for the foreman to control all the movements while the helper carried out other tasks. In this occurrence, the crew followed this practice of the foreman controlling all the movements.
1.18.1 Railway Employee Qualification Standards Regulations
In Canada, the Railway Employee Qualification Standards Regulations (the Regulations), which came into force in 1987, establish the minimum qualifications for LEs, transfer hostlers, conductors, and yard foremans. They apply to all federally regulated railway employees performing the duties of the specified occupational category (Appendix B).
Since the Regulations came into force, there have been significant operational changes in the rail industry, including crew size being reduced and RCLS operations being widely implemented across the country. Despite these significant changes in railway operations, the Regulations have not been modified in more than 30 years.
At the time the Regulations came into force, operating employees typically followed a graduated promotion approach from brakeman / yard helper to conductor / yard foreman, and then to LE. As the industry and technology evolved, the role of brakeman was phased out and new operating employees were typically hired as conductor trainees. As a result, when the new employees completed their conductor training, they were considered qualified as yard helper, conductor, and yard foreman. Over the years, training delivery has changed, to the point that some new conductor candidates can now qualify within 6 months.
Training programs for operating occupational categories, such as RCLS operators and rail traffic controllers (RTCs), are not covered by the regulations, but most railways have training plans and manuals in place for those positions.
The Railway Safety Act review panel examined the training and qualification issue in its report entitled Stronger Ties: A Shared Commitment to Railway Safety – Review of the Railway Safety Act, which was released in 2007. The panel examined the Railway Employee Qualification Standards Regulations as they related to operating employee qualification standards, graduated qualification, training, and regulatory oversight. The review panel’s report identified the fact that the regulatory framework for railway employee qualification had not kept pace to reflect the significant changes in the railway operating environment.
The training and qualification issue was examined again by the 2018 Railway Safety Act review panel. Its report entitled Enhancing Rail Safety in Canada: Working Together for Safer Communities included the following observations and conclusions:
The 2007 RSA Review looked at training for operating crews and ultimately refrained from making a recommendation on the matter, as it recognized that although the applicable regulations had not been updated since 1987, industry programs are updated on an ongoing basis and monitored by Transport Canada, which is still the case today.68 […]
Although Transport Canada certifies aviation and marine crew members, there are no provisions for certifying railway employees or approving railway training programs. As such, each company is awarded considerable latitude in preparing and providing training and certification tailored to the specific needs of its employees. The Review heard from some Transport Canada inspectors that they occasionally note gaps in the consistency of training (e.g., knowledge) of railway personnel, and while CN and CP have taken steps to address training gaps through company training centres in Winnipeg and Calgary, further efforts could be made to strengthen training requirements of railway personnel. […]
[…] The Review is satisfied and encouraged by Transport Canada’s current efforts to update and broaden its approach to the railway employee qualification and training framework, with a view to revising/replacing the existing regulations. This is an important undertaking, given the number of railway industry changes in the areas of new technology, increased staff turnover, and associated new hires.
_________
68 2007 Railway Safety Act Review. Stronger Ties: A Shared Commitment to Railway Safety, Review of the Railway Safety Act. November 2007. pp. 163–164.Footnote 37
1.19 TSB Railway Investigation Report R16T0111 and Recommendation R18-02
On 17 June 2016, at about 2335 Eastern Daylight Time, the CN RCLS 2100 west industrial yard assignment was performing switching operations at the south end of CN’s MacMillan Yard in Vaughan, Ontario. The assignment, handling 72 loaded cars and 2 empty cars, was 4537 feet long and weighed 9116 tons. The assignment was pulling southward from the yard onto the York 3 main track in order to clear the switch at the south end of the Halton outbound track to gain access to the west industrial lead track (W100) switch. The assignment helper attempted to stop the assignment to prepare to reverse into track W100, in order to continue switching for customers. However, the assignment could not stop and continued to roll uncontrolled for about 3 miles, reaching speeds of up to 30 mph before stopping on its own at about Mile 21.1 of the York Subdivision. There were no injuries. There was no release of dangerous goods and no derailment.
The investigation highlighted deficiencies in the current Railway Employee Qualification Standards Regulations. The Board noted that TC’s 2017–18 Departmental Plan highlighted its intention to update the Railway Employee Qualification Standards Regulations, but there had been little progress to date. Consequently, the regulations had not kept pace with the significant changes in railway operations over the years. The Railway Safety Management System Regulations, 2015, which require railways to have processes for managing knowledge, covered some of the training elements. However, gaps in training remained.
If the gaps in the current Railway Employee Qualification Standards Regulations were not addressed, railway employees in safety-critical positions might not be sufficiently trained or experienced to perform their duties safely. Additionally, TC would not be able to conduct effective regulatory oversight and enforcement of training programs. Therefore, the Board recommended that
the Department of Transport update the Railway Employee Qualification Standards Regulations to address the existing gaps for railway employees in safety-critical positions related to training, qualification and re-qualification standards, and regulatory oversight.
TSB Recommendation R18-02Footnote 38
1.19.1 Transport Canada’s latest response to TSB Recommendation R18‑02 (December 2019)
In December 2019, Transport Canada provided an update to its response to the recommendation. It stated the following:
The Department continues work to improve its regulatory regime for railway employee qualification and training regime. Transport Canada published in 2019 the Guideline for Remote Control Locomotive Operation. The guideline, which is available on the department’s website (https://www.tc.gc.ca/eng/railsafety/guideline-78.html), makes recommendations in the area of training and qualification for employees involved in remote control locomotive (RCL) operations.
More broadly, the Department’s objective is to ensure Canada’s federally-regulated railway companies have training programs that adequately train their employees for safe railway operations. To this end, the Department consulted with stakeholders, and conducted site visits to observe best practices with respect to training programs. In addition, the Transport Canada reviewed Transportation Safety Board (TSB) data on rail occurrences to better understand the role that the lack of training played in incidents and accidents as well as reviewing the regulatory regimes in the United States, Australia and E.U. on employee training.
During 2020, Transport Canada will begin consultations with stakeholders on policy options for amendments to the Railway Employee Qualification Standards Regulations, with draft regulations to follow sometime in –21.
While this work is underway, Transport Canada will continue to oversee railway companies’ obligations with respect to training under the Railway Safety Management System Regulations, 2015.Footnote 39
1.19.2 Board reassessment of Transport Canada’s response to TSB Recommendation R18-02 (March 2020)
In March 2020, the Board reassessed TC’s response to Recommendation R18-02 and stated the following:
The Board assesses the response to Recommendation R18-02 as having Satisfactory Intent.Footnote 40
1.20 Guideline for Remote Control Locomotive Operation
In April 2019, TC published a Guideline for Remote Control Locomotive Operation, which “promotes industry best practices and provides federally regulated railways, and those providing services to railways, with guidance on the continued safe use of remote control locomotives (RCLs).” Footnote 41
The guideline addresses training, qualifications, compliance, and operational parameters. With regard to the initial training of employees, the guideline suggests that employees receive training on RCLS-controlled locomotive operation, air brake operation, and train handling, and that they gain an understanding of forces acting on the movement and train handling techniques in various weather conditions and grades.
With regard to crew experience, Section 1.1 of the guideline indicates that consideration should be given to:
- Implementing RCL training and qualification programs separately from training for other occupational categories (e.g., conductor training)
- Establishing separate RCO qualification standards for yard and outside-of-yard operations (“outside of yard” includes main track, spurs and subdivision track)
- Ensuring an RCO operating an RCL outside of a yard is trained to have equivalent competencies as a locomotive engineer
- Establishing criteria, such as minimum experience of each crew member and amount of supervision required, for when less experienced RCOs may work together
- Criteria should take into account the job position (conductor or assistant conductor), and whether the work is happening in a yard or outside of a yard Footnote 42
Section 2.2, Establishing operational parameters, recommends that railways
- Develop instructions, in collaboration with labour, and based on an assessment of risk, for all locations where RCLs are operated (including yards, spurs, subdivisions and main tracks)
- Examples of parameters to use in the analysis:
- grade at the location, in each direction of travel
- locomotive axle count and horsepower
- train length and tonnage
- types of rail cars and equipment
- method of complying with CROR [Canadian Rail Operating Rules Rule] 115
- Standardize RCL speed to a maximum of 15 mph, to reflect current operating practices
- Have procedures in place that guide employees to work safely in the event one of the two OCUs fails during a shift (for example, the RCO with the working OCU has direct sight of the other crew member)
- Note: If this happens, the railway should use all reasonable means to immediately replace the inoperative OCU
- Have minimum standards for air to be used through every rail car outside of yards with RCL operation, regardless of the method of control
- Ensure RCLs outside of yards have features that allow the RCO to apply the air brakes while under tractive effort, to better allow them to control the RCL’s movement Footnote 43
1.21 Railway Safety Management System Regulations, 2015
On 01 April 2015, the Railway Safety Management System Regulations, 2015 (SMS Regulations) came into force and replaced the 2001 SMS Regulations. Under these regulations, federally regulated railway companies must develop and implement a safety management system (SMS), create an index of all required processes, keep records, notify the Minister of Transport of proposed changes to their operations, and file SMS documentation with the Minister when requested.
1.21.1 Risk management
The SMS Regulations state that, among other things, railway companies
must develop and implement a safety management system that includes […]
(e) a process for identifying safety concerns;Footnote 44 […]
(g) a process for implementing and evaluating remedial actionFootnote 45 [...].Footnote 46
Section 13 of the SMS Regulations states the following:
A railway company must, on a continual basis, conduct analyses of its railway operations to identify safety concerns, including any trends, any emerging trends or any repetitive situations. The analyses must, at a minimum, be based on
- any reports of railway occurrences;
- any internal documentation relating to railway occurrences;
- any reports of injuries;
- the results of any inspections conducted by the railway company or by a railway safety inspector;
- any reports of contraventions or safety hazards that are received by the railway company from its employees;
- any complaints relating to safety that are received by the railway company;
- any data from safety monitoring technologies;
- the conclusions of the annual report referred to in subsection 29(3); and
- the findings of any audit reports.Footnote 47
Section 15 of the SMS Regulations lists the circumstances in which railway companies must conduct a risk assessment. One of these circumstances is “when it identifies a safety concern in its operations as a result of the analysis conducted under section 13.”.Footnote 48
In accordance with the SMS Regulations, CN has developed and implemented a detailed SMS. CN’s SMS has been enhanced every year since 2008 and integrated into most facets of its operations. It describes company initiatives that correlate to the requirements of section 2 of the SMS Regulations.
CN’s Risk Assessment Standard states that risk assessments shall be performed in the following instances:
- Changes to operations, procedures, infrastructure, technology, etc.
- Trend analysis showing a gradual deterioration or a sudden increase.
- Issues identified through injury and accident investigations, investigations, complaints, inspections, etc.Footnote 49
If a risk assessment is determined to be necessary, the Risk Assessment Standard defines the steps to be followed, which include identifying hazards, assessing hazards, selecting control measures or remedial action, and implementing the control measures or remedial action.Footnote 50.
1.21.2 Reporting contraventions, safety hazards, and close calls
With regard to reporting contraventions or safety hazards, subsections 24(1) and (2) of the SMS Regulations state the following:
Internal reporting
24 (1) A railway company must include, in its safety management system, a procedure for enabling its employees to report to the railway company, without fear of reprisal, a contravention of the Act or of any regulations, rules, certificates, orders or emergency directives made under the Act in relation to safety, or a safety hazard.
Policy
(2) The railway company must include, in its safety management system, a policy, in writing, for protecting its employees from reprisals for reporting a contravention or safety hazard.Footnote 51
Although the regulations do not specifically mention close calls, some railway companies have begun to implement close-call reporting systems. For example, VIA Rail Canada Inc. (VIA Rail) crews are encouraged to self-report instances of close calls or rule violations with the understanding that there will be no discipline, or discipline will be reduced, if the crew self-identifies.
In 2013, CN established an independent close-call reporting hotline for employees called PREVENT, which was managed through St. Mary’s University in Halifax, Nova Scotia. Employees were encouraged to call in to self-report near misses and close calls. St. Mary’s University edited the data to ensure that the reports remained confidential. The results were then shared with management for corrective action when warranted. However, the program met with limited success and ceased operation in 2017.
Under CN’s SMS Procedure and Policy for Reporting Contraventions or Safety Hazards, employees are instructed to report all safety hazards and concerns to local management. Under this procedure, employees who want to report a contravention or safety hazard without fear of reprisal are instructed to contact the CN Ombudsman’s office. From 2009 to 2018 inclusive, the ombudsman’s office received 147 confidential reports related to safety.
To encourage occurrence reporting, a number of international jurisdictions have set up confidential rail safety reporting systems that offer reporters confidentiality and protection from prosecution.
1.21.2.1 Federal Railroad Administration and National Aeronautics and Space Administration Confidential Close Call Reporting System
The U.S. Federal Railroad Administration (FRA) set up a program known as the Confidential Close Call Reporting System C3RSFootnote 52 in 2007. Following a pilot program involving 4 railroads, each participating for a period of 5 years, the program was opened to other operators. As of 2018, 8 railroads were participating in the program; however, participants consist of passenger railroads only.Footnote 53
Railroads participate under a memorandum of understanding (MOU). Specific provisions can vary, but generally include the following:
- An employee has a defined period to file a report with C3RS for a close call. A close call is defined as “any condition or event that may have the potential for more serious safety consequences.”Footnote 54
- Reports are sent directly to the National Aeronautics and Space Administration (NASA), which servesas the “honest broker” (an objective third party). Once NASA has reviewed the reports, it may contact the submitter for additional information. Following this, reports are de-identified and an identification strip on the report is sent back to the submitter as proof that a report has been filed.
- Filing a report protects the submitter from company and FRA disciplinary action in most circumstances (as set out in the MOU).
- De-identified reports are analyzed by a peer-review team that includes company and FRA representatives.
C3RS is complementary to, and does not replace, other safety reporting programs such as those provided by a company’s safety management structure. A review of C3RS by the FRA identified the following:
- C3RS has demonstrated bottom-line impacts in the reduction of derailments, injuries, discipline hearings, and equipment costs.
- Effective labour and management relations had a positive impact on safety culture.
- The improvement in safety culture was perceived to have increased the communication between supervisors and labour in the presence of C3RS, in particular when supervisors embrace the willingness to communicate and have productive, blame-free conversations about safety with their employees.
- Improved cooperation between labour and the organization helped achieve more systemic corrective actions.
- The review team had limited opportunities to collect additional safety data related to reported occurrences from the organizations. Therefore, it could not provide a greater understanding of all contributing causes and potential corrective actions.
- Railways can share knowledge about non-proprietary process improvements and corrective actions, increasing the overall benefit of C3RS in the industry.
- An increase was identified in the initiation of corrective actions following occurrences. However, a more robust tracking feature is needed to monitor the effectiveness of the corrective actions.Footnote 55
1.21.2.2 United Kingdom’s Confidential Incident Reporting and Analysis Service
The United Kingdom’s Confidential Incident Reporting and Analysis Service (CIRAS)Footnote 56 was established in 1996. It provides an independent, confidential safety reporting line for various transportation industries, including bus and rail.
The CIRAS is governed by the CIRAS Committee, which consists of representatives from the United Kingdom rail industry and other United Kingdom transportation modes. The committee also includes a number of trade union members and independent professionals with expertise in other industries (such as oil and gas), as well as academic researchers. The program shares lessons learned with all industries through newsletters and information on its website.
The CIRAS reporting and follow-up process is similar to the FRA’s C3RS program, with CIRAS serving as an “honest broker”. Once a report is submitted (i.e., through the website, or by text, phone, or hard copy), the submitter is contacted outside of work to obtain additional information, and a report is prepared and submitted to the appropriate member organization. A response is then provided to the submitter outlining any action taken.Footnote 57
1.21.2.3 TSB confidential reporting program
The TSB administers a program called SECURITAS that enables confidential reporting on concerns about safety in the air, marine, pipeline, and rail modes of transportation. The incidents and potentially unsafe acts or conditions submitted through SECURITAS are not always reported through other channels (nor are they required to be).
SECURITAS reports can lead to the TSB issuing safety communication letters to the Minister of Transport, to other government departments, or to industry organizations for action. These reports can also help the TSB identify widespread safety issues. By combining confidential report data with other accident and incident reports and studies, and by sharing safety information with other agencies in Canada and abroad, a greater insight is gained into national and global transportation safety issues. SECURITAS reports can also support TSB studies and analyses on safety-related matters such as operating procedures, training, human performance, and equipment.
1.21.3 Managing knowledge
Paragraph 5(k) and subsection 28(1) of the SMS Regulations state, in part, that a railway must have a process with respect to scheduling. The scheduling process outlined in the regulations requires that the company apply the principles of fatigue science when scheduling the work of operating employees. There is no requirement to consider the experience of operating employees who may be paired together for work.
With regard to crew training, sections 25 to 27 of the SMS Regulations require a railway to have a process for managing knowledge. Section 25 of the SMS Regulations states that
25(1) A railway company must establish a list setting out
- the duties that are essential to safe railway operations;
- the positions in the railway company that have responsibility for the performance of each of those duties; and
- the skills and qualifications required to perform each of those duties safely.Footnote 58
Section 27 states that a railway company must also include in its SMS a plan for ensuring that employees who perform any of the duties in the list mentioned in subsection 25(1) have the skills, knowledge, and qualifications required to perform their duties safely,Footnote 59 as well as a method for verifying this.Footnote 60
In accordance with these sections of the SMS Regulations, CN had a process document outlining its plan for managing knowledge, entitled SMS-CN Process for Managing Knowledge. The document contained the lists required by subsection 25(1) and the plan and methods required by section 27 of the regulations. In addition to the conductor, LE, and RCLS operator positions, the CN list included other operational positions. The SMS Regulations do not require individual plans and methods for each position, and do not prescribe the training requirements to qualify for each position.
With regard to employees performing train operations, CN identified the duties essential to safe railway operations and the positions performing the duties:
- Operating a train: conductor
- Operating a locomotive: LE, RCLS operator,Footnote 61 conductor locomotive operator, and hostler
- Controlling train movement: RTC
For each position, the skills and qualifications required to perform essential duties were listed in Annex A – Employees Skills and Qualifications, which outlined the training requirements of the positions. A review of the document revealed that
- there is no minimum experience requirement to operate as yard foreman and RCLS operator;
- conductors and RCLS operators do not receive train simulator, train handling, or locomotive operation training;
- there is no requirement for RCLS operators to requalify in RCLS operation; and
- RCLS operators must have 40 hours of practical training with field sign-off.
1.22 Crew resource management
Crew resource management (CRM) focuses on providing crews with the interpersonal skills required to carry out their tasks safely: “CRM training typically consists of an ongoing training and monitoring process through which personnel are trained to approach their activities from a team perspective rather than from an individual perspective.”Footnote 62
Significant safety benefits were experienced in the aviation and marine industries with the introduction of CRM and bridge resource management, respectively. Given the prevalence of human factors in rail accident statistics, this type of training could yield significant safety benefits in the rail industry.Footnote 63
Following a 1998 collision between 2 freight trains, the U.S. National Transportation Safety Board (NTSB) recommended that a number of railway stakeholders, including the regulator, operators, industry associations, and labour organizations, collaborate to develop and require CRM training in the railway industry. That training would cover, at a minimum, crew member proficiency; situational awareness; effective communication and teamwork; and strategies for appropriately challenging and questioning authority.Footnote 64
Subsequent to this recommendation, the FRA, in cooperation with academic and industry partners, developed and piloted rail CRM training.Footnote 65 Initial assessment of the pilot training showed increases in knowledge and improved attitudes toward CRM principles.Footnote 66
However, this type of training has not been made mandatory in either Canada or the U.S. A review of the adaptation of CRM principles outside of aviation in 2010 found that, in the North American railway industry, “interest in CRM training principles remains sporadic.”Footnote 67 The review also described voluntary initiatives by specific railways to implement CRM training, as well as industry initiatives to develop training materials for operators to use. For example, the review indicated that Canadian Pacific Railway (CP) implemented a CRM training program targeted at new-hire conductors and trainmen in 1999.
A similar initiative in the United Kingdom involved the definition of non–technical skills for railway crew. The Rail Safety and Standards Board (RSSB) published a best practices guide for developing non-technical skills. The guide specifies 7 areas of non-technical skills that have been shown to be critical to performance in safety-critical roles:
- Situational awareness
- Conscientiousness
- Communication
- Decision making and action
- Cooperation and working with others
- Workload management
- Self-managementFootnote 68
1.22.1 VIA Rail Canada Inc. locomotive cab awareness training
Since 2013, VIA Rail Canada Inc. has been providing all its LEs with an 8-hour course known as locomotive cab awareness. The objective of the course is to improve safety by providing LEs with the principles of CRM.
The training focuses on acquiring the skills necessary to gain and maintain awareness. This enables the trainee to avoid the traps associated with the loss of awareness, and to better cope with unexpected and hazardous situations by improving crew interactions in the locomotive cab.
1.22.2 Canadian National Railway Company’s assessment of communication and coordination during conductor training
CN does not provide conductors with formal rail CRM training. However, the conductor trainee evaluation form used at CN includes behavioural indicators to help trainers assess communication and coordination among crew members. For example, the form sets out the expectation that the conductor trainee will participate in job briefings, and will have a clear understanding of tasks to be performed and safety hazards identified.
With respect to peer-to-peer communication between crew members, the form sets out the expectation that a conductor trainee will communicate in specific situations (e.g., derails applied or removed, switches lined, hand brakes applied), and will participate in ongoing job briefings, and communicate restrictions and changes in plans. The form also includes an overall assessment of initiative, confidence, and cooperation with co-workers.
1.23 Safety culture
All members of an organization, and the decisions made at all levels, have an impact on safety. A recognized definition of an organization’s “safety culture” is
shared values (what is important) and beliefs (how things work) that interact with an organization’s structures and control systems to produce behavioural norms (the way we do things around here).Footnote 69
The relationship between safety culture and safety management is reflected in part by the beliefs, attitudes, and behaviours of a company’s management.
An effective safety culture includes proactive actions to identify and manage operational risk. It is characterized by an informed culture, in which people understand the hazards and risks involved in their own operation, and work continuously to identify and overcome threats to safety. It is a just culture, in which the workforce knows and agrees on what is acceptable and unacceptable. It is a reporting culture, in which safety concerns, including close calls, are reported and analyzed, and appropriate action is taken. Finally, it is a learning culture, in which safety is enhanced from lessons learned.Footnote 70
A company’s policies determine how safety objectives will be met by clearly defining responsibilities; by developing processes, structures, and objectives to incorporate safety into all aspects of the operation; and by developing the skills and knowledge of personnel. Procedures are directives for employees, and they communicate management’s instructions. Practices are what really happens on the job, which can differ from procedures and, in some cases, increase threats to safety.
In April 2016, the TSB held a Transportation Safety Summit that brought together more than 70 senior executives and leaders representing operators, labour organizations, industry associations, and regulators from all modes of transportation. Through a combination of presentations, expert panels, and facilitated working groups, the summit provided a forum to hear experiences and best practices, and to exchange and challenge ideas about how to encourage information flow to improve safety.
A broad consensus emerged from the discussions: to effectively improve safety, an SMS must clearly identify the systemic issues underlying behaviour. Further, effective communication and collaboration were key elements in building the trust necessary to address safety issues at this level. However, the biggest challenge identified in terms of bringing about this type of just culture was the need to build trust and respect in organizations that may have a history of blame.Footnote 71
1.24 Safety culture at Canadian National Railway Company
In parallel with implementing an SMS, CN has recognized the importance of building an effective safety culture, which the company considers essential for SMS. To help strengthen its safety culture, CN has invested in training, coaching, employee recognition, and involvement.
In 2014, CN opened 2 new training centres—1 in Winnipeg, Manitoba, and 1 in Homewood, Illinois, U.S. Both centres offer courses for new and seasoned railroaders, from conductor to car mechanic and from track inspector to signal maintainer. Employees receive hands-on training in modern indoor laboratories with up-to-date equipment. CN estimated that some 3000 employees per year would be trained at the new centres.
In October 2014 and October 2017, CN co-hosted a safety culture symposium in Halifax, Nova Scotia, where attendees discussed and shared information about the emerging field of safety culture. CN also hosts safety summits throughout its territories to promote two-way communication and best safety practices.
CN has also been integrating the just culture model into its discipline policy. In some situations, employees could be subject to discipline if they are involved in an operating incident. However, when applying the just culture model, involvement in multiple operating incidents may not necessarily result in an employee being disciplined. Rather, an employee would not be disciplined if, despite their good intentions, an incident occurred.
Among other initiatives, in 2014, CN developed and implemented Looking Out for Each Other, a peer-to-peer engagement strategy designed to
- raise awareness among employees of the top causes of incidents and injuries;
- identify and review safe work procedures for those activities;
- train employees to be aware of their surroundings, and to recognize potential at-risk work practices or situations in the field;
- teach employees how to provide constructive feedback to peers; and
- learn from past incidents to prevent a recurrence of the same event and help each other stay safe.Footnote 72
1.24.1 Partners in Prevention
Partners in Prevention is a CN program intended to modify behaviour by encouraging communication between employees and company officers. Under the program, trainmasters are expected to perform 1 test per shift that may include employee meetings at the start of shifts, observations, or field testing. Results are shared between the employees, the union, and the company and can result in coaching, verbal feedback, or group discussions. The program is intended to replace a punitive system that relies on disciplinary action to encourage safe behaviours.
At Melville Yard, the experience with the Partners in Prevention program was generally positive, and resulted in improved communication among operating employees with respect to the interpretation and application of rules.
1.25 Other TSB investigations involving training or experience while switching using remote control locomotive systems
Since 2007, the TSB has investigated 5 other occurrences involving RCLS switching operations (Appendix C), in which the inexperience of (an) operating crew member(s) involved in switching and using remote control locomotive systems contributed to the occurrence:
- TSB Railway Investigation Report R16T0111 determined that operating crew inexperience and insufficient training played a role in the occurrence.
- TSB Railway Investigation Report R16W0074 determined that operating crew inexperience played a role in the occurrence.
- TSB Railway Investigation Report R07T0270 determined that crew inexperience and inadequate training contributed to the occurrence.
- TSB Railway Investigation Report R07V0213 determined that management crew inexperience, inadequate management crew training, and the implementation of an operational change related to RCLS switching operations contributed to the accident. Although a risk assessment was conducted for the change involved, it was inadequate to identify all the hazards and mitigate the risks of switching long, heavy cuts of cars on a descending grade.
- TSB Railway Investigation Report R07W0042 determined that crew inexperience, inadequate training, and some form of distraction that occurred while conducting RCLS switching operations contributed to the accident.
1.26 TSB occurrence statistics involving unplanned/uncontrolled movements
From 2009 to 2018, there were 562 occurrencesFootnote 73 reported to the TSB related to unplanned/uncontrolled movements among all railways in Canada (Table 2).
| Reason for unplanned or uncontrolled movement | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Loss of control | 0 | 2 | 3 | 0 | 3 | 0 | 1 | 4 | 2 | 5 | 20 |
| Switching without air | 14 | 10 | 16 | 12 | 24 | 21 | 22 | 18 | 21 | 27 | 185 |
| Securement | 37 | 25 | 32 | 44 | 42 | 38 | 37 | 29 | 39 | 34 | 357 |
| Total | 51 | 37 | 51 | 56 | 69 | 59 | 60 | 51 | 62 | 66 | 562 |
Note: The data summarizing the number of uncontrolled movements each year have not been adjusted for variations in annual rail traffic volumes.
Uncontrolled movements generally fall into 1 of 3 causal categories:
- Loss of control: when an LE or an RCLS operator cannot control a locomotive, a car, a cut of cars, or a train with available locomotive and/or train air brake systems.
- Switching without air: when a movement is switching with the use of the locomotive independent brakes only, with no air brakes available on the cars being switched or kicked. The vast majority of these incidents occur in yards.
- Securement: When a car, a cut of cars, or a train is left unattended and begins to roll away uncontrolled, usually because
- an insufficient number of hand brakes have been applied to a car, a cut of cars, or a train; and/or
- a car (or cars) has faulty or ineffective hand brakes.
Of the 562 occurrences:
- Loss of control was the causal category in 20 (4%) of the occurrences.
- Switching without air, as in this occurrence, was the causal category in 185 (33%) of the occurrences.
- Insufficient securement was the causal category in 357 (63%) of the occurrences.
Kendall’s τb correlation coefficientFootnote 74 was calculated on the overall number of uncontrolled movements by year from 2009 to 2018. There was a strong positive correlation indicating an upward trend in occurrences involving unplanned/uncontrolled movements overall (τb = 0.5521, p = 0.0293). Based on Sen’s estimate of slope, Footnote 75 the average increase per year for all categories was 1.67 occurrences per year (Figure 17).
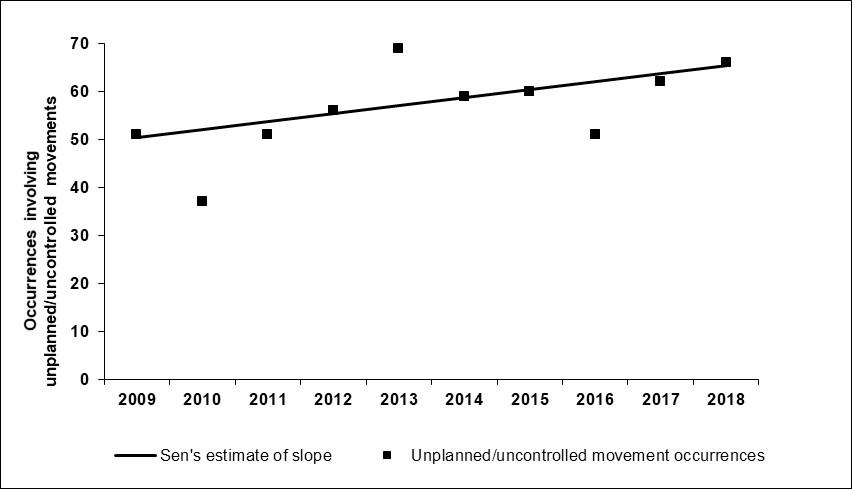
Kendall’s τb correlation coefficient was then calculated on the 3 categories (see Table 2) by year from 2009 to 2018. Of the 3 categories, only switching without air showed a significant increase over the period. There was a strong positive correlation indicating an upward trend in occurrences involving unplanned/uncontrolled movements that occurred while switching without air. Based on Sen’s estimate of slope, the average increase per year was 1.44 occurrences per year (Figure 18). These estimates indicate that 86% of the 10-year annual increase in overall occurrences involving unplanned/uncontrolled movements was associated with switching without air.
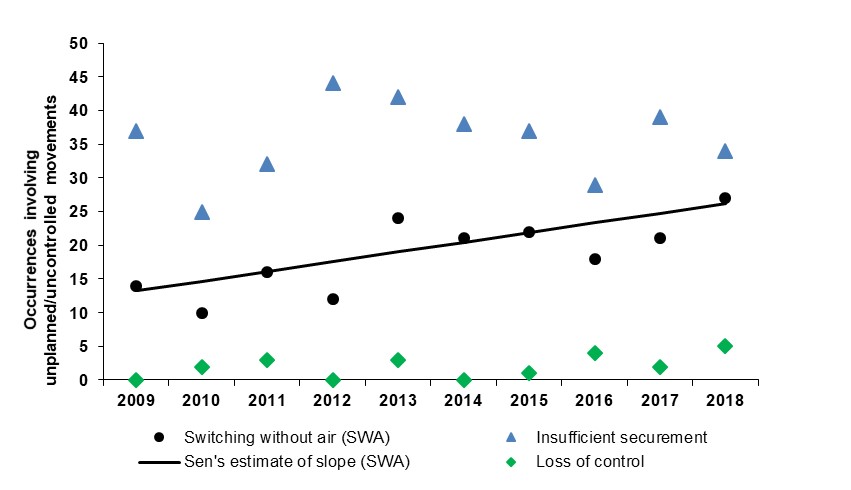
Of the 185 uncontrolled movements that occurred while switching without air,
- 70 (37.8%) occurred as a result of rollbacks,
- 134 (72.4%) resulted in a collision, and
- 56 (30.3%) involved dangerous goods.
Table 3 provides a breakout by consequences.
| Consequence* | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Total | % of total switching without air occurrences |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Derailment of 1 to 5 cars | 7 | 4 | 8 | 3 | 6 | 5 | 8 | 12 | 7 | 11 | 71 | 38.4% |
| Derailment of more than 5 cars | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 2 | 5 | 2.7% |
| Collision | 13 | 9 | 13 | 10 | 19 | 15 | 17 | 7 | 16 | 15 | 134 | 72.4% |
| Affected the main track** | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 2 | 1 | 0 | 7 | 3.8% |
| Involved dangerous goods | 5 | 3 | 4 | 0 | 4 | 10 | 8 | 5 | 7 | 10 | 56 | 30.3% |
| Injuries or fatalities | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 2 | 1.1% |
* Some occurrences may have more than one consequence.
** Originated on the main track, moved onto the main track, or fouled the main track.
Since 1994, in addition to this occurrence, the TSB has investigated 32 other occurrences that involved uncontrolled movements (Appendix D), 7 of which were related to switching without air.
1.27 Previous recommendation and safety concern involving uncontrolled movements
As a result of the TSB investigation into the July 2013 Lac-Mégantic accidentFootnote 76, the Board recommended that
the Department of Transport require Canadian railways to put in place additional physical defences to prevent runaway equipment.
TSB Recommendation R14-04Footnote 77
This recommendation primarily dealt with inadequate securement of rolling stock. In response, Transport Canada (TC) implemented a number of initiatives, including strengthening securement requirements in Canadian Rail Operating Rules (CROR) Rule 112 and introducing a comprehensive oversight plan for the new rule. In March 2020, the Board reassessed TC’s response to Recommendation R14-04 to be Satisfactory in Part.
As a result of an investigation into the March 2016 uncontrolled movement of equipment that travelled onto the main track in Saskatoon, Saskatchewan, it was determined that, despite TC and industry initiatives, the desired outcome of significantly reducing the number of uncontrolled movements has not yet been achieved. Consequently, the Board issued the following safety concern:
The Board is concerned that the current defences are not sufficient to reduce the number of uncontrolled movements and improve safety.Footnote 78
1.28 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer.
Safety management and oversight is a Watchlist 2018 issue. All transportation companies have a responsibility to manage safety risks in their operations.
While some companies consider safety to be adequate as long as they are in compliance with regulatory requirements, regulations alone cannot foresee all risks unique to a particular operation. That is why the TSB has repeatedly emphasized the advantages of SMS, an internationally recognized framework to allow companies to effectively manage risk and make operations safer.
In this occurrence, the employees at Melville Yard were aware that uncontrolled movements, including rollbacks, were common in the area of the accident. However, the railway was only aware of the accidents in which the uncontrolled movements resulted in a collision and/or derailment. Other uncontrolled movements in the area were not reported and therefore could not be analyzed.
ACTIONS REQUIRED Safety management and oversight will remain on the Watchlist until:
|
Without effective non-punitive incident reporting, data pertaining to incidents involving close calls may not be consistently collected. Therefore, the opportunity to perform leading indicator analysis and implement appropriate mitigation measures may be lost.
1.29 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP041/2018 – Hand Brake Ratio Calculation
- LP021/2020 – Braking Distance Calculations
2.0 Analysis
The condition of the track did not play a role in this occurrence. The analysis will focus on kicking cars and switching without air in Melville Yard; the effectiveness of the hand brake on car CN 302412; the assignment crew’s switching plan, communication, experience, and coordination of activities; inspection of similar cars; safety management systems (SMS); close-call reporting; and the increase in unplanned/uncontrolled movements.
2.1 The accident
In preparation for placing three 44-foot-long open-top hopper cars loaded with ballast (CN 302369, CN 90393, and CN 302412) into track MR13, the foreman returned with the assignment to the MR-lead track just east of the MR19 switch and lined the switch for the MR-lead track. The helper walked back to the cars that were already stationary in track MR13, positioned about 50 feet from the fouling point of the MR-lead track.
The helper stayed with the cars in track MR13, anticipating that the assignment would enter track MR13 and make a joint to push the stationary cars westward. From the helper’s location, the eastward view of the MR-lead track was blocked by stationary cars in an adjacent track. There was no specific communication between the crew members. The helper was unaware that the foreman intended to kick the 3 open-top hopper cars into track MR13, rather than shoving them to couple with the stationary cars in MR13 and pushing all the cars westward.
The foreman had been kicking cars at 7 mph for most of the shift. The foreman uncoupled the 3 open-top hopper cars loaded with ballast (the 3 cars), selected a speed of 7 mph on the Beltpack, and shoved westward before stopping. As the assignment stopped, the 3 cars separated from the assignment and travelled under their own momentum on the MR-lead track toward track MR13.
The foreman then lined the MR19 switch and reversed the assignment into the track. After doing so, the foreman noticed that the 3 cars had stalled on the MR-lead track and begun to roll back toward the assignment. The foreman made a radio broadcast indicating that the 3 cars were rolling back. The helper, standing beside the lead car in track MR13 and not in a position to intervene, heard the radio broadcast and ran toward the uncontrolled movement.
At 1802:57, the foreman made an independent brake application and the assignment came to a stop 7 seconds later (at 1803:04), with lead car PLCX 21492 partially in track MR19 but still foul of the MR-lead track. After initiating the independent brake application, she ran from the MR19 switch to the leading B end of the uncontrolled movement’s lead car CN 302412. The foreman reached the car and climbed the ladder that extended to the CN 302412 B-end platform to access the high-mounted hand brake.
Once on the platform, the foreman applied the hand brake, but the southeast corner of CN 302412 collided with the northwest corner of stationary, empty covered hopper car PLCX 21492.
The accident occurred when 3 open-top hopper cars loaded with ballast were kicked up an ascending grade on the MR-lead track, stalled, rolled back, and collided with the lead car of the assignment, empty car PLCX 21492, which was foul of the lead track. While attempting to stop the uncontrolled cars by applying the hand brake on CN 302412, the foreman became pinned between PLCX 21492 and CN 302412, receiving fatal injuries.
2.2 Hand brake effectiveness
Post-accident examination of the B end of CN 302412 identified that the hand brake chain, connecting rod, and bell crank were not in their proper positions. The large connecting chain link had pulled up close to the hand brake housing and there was no white paint visible on the hand brake chain. In addition, the hand-brake connecting rod and the bell crank were pulled tight against the end sill. This indicates that, prior to the collision, the hand brake wheel on CN 302412 had been turned beyond what was required to fully apply the hand brake.
Following the accident, when the hand brake was released, the bell-crank bracket and bell crank fell away from the car. The welds securing the bell-crank bracket to the underside of the B-end sill of CN 302412 had failed. As the fracture surfaces on the welds were heavily corroded, the corrosion had likely been present (yet undetected) for an extended period of time. The rear of the outboard welds’ fracture surfaces and the corresponding bell-crank bracket fracture surface each contained small zones of more recent fresh fracture. Given the absence of any impact damage to the bell-crank bracket, it is probable that the welds failed when the hand brake force applied under normal conditions exceeded the strength of the remaining reduced cross-sectional area of the welds.
A hand-brake effectiveness test, performed the day after the accident with the components in the as-found condition and the hand brake fully applied, determined that the hand brake was ineffective and could not hold the 3 cars. Subsequent brake-shoe force testing determined that a hand brake with rigging in this condition is ineffective, and would have had little or no effect in slowing or stopping the cars. When the foreman applied the hand brake, the welds securing the bell-crank bracket to the underside of the B-end sill of CN 302412 failed and the bell crank and the bracket separated from the car, rendering the hand brake ineffective.
2.2.1 Stopping distance calculations
TSB calculations identified that the force of 1 fully functioning hand brake, if properly applied, would be sufficient to stop the 3 cars on the 0.5% descending grade.
The TSB re-enactment identified that it took 22 to 30 seconds for the cars to travel to the point of impact after they began to roll back. On average, it took about 18 seconds for a person to react and run from the north side of the MR19 switch (i.e., where the foreman was positioned) to the location of car CN 302412, estimated to be about 50 feet away, to climb the ladder to access the hand-brake end platform, and to fully apply the hand brake.
Based on the TSB on-site re-enactment, when the cars started to roll back, during the 18 seconds that it took a person to react and fully set the hand brake, the cars would have reached a speed of about 1.72 mph and traveled a distance of 22.7 feet during that time. This calculation assumes the hand brake would have been completely ineffective until it was fully applied, whereas the car would have actually begun to slow as the hand brake was applied.
If the hand brake had been fully applied using 125 foot-pounds of torque and had been fully effective, the 3 cars would have come to a stop within an additional 21.2 feet.
Although there are a number of unknown factors and estimated distances, the combined total for the calculated travel distance (22.7 feet) and stopping distance (21.2 feet) would be 43.9 feet, which is 6.1 feet less than the estimated 50 feet of distance to car CN 302412. Once the hand brake was fully applied, a fully effective hand brake on car CN 302412 could have stopped the uncontrolled movement within the available distance.
However, when the foreman applied the hand brake, the welds securing the bell-crank bracket to the underside of the B-end sill of CN 302412 failed and the bell crank and the bracket separated from the car, rendering the hand brake ineffective.
Because the braking efficiency of the hand brake was compromised, the uncontrolled movement did not stop or slow, which reduced the opportunity and time for the foreman to safely egress.
2.2.2 Safety appliance inspection
Two days before the occurrence, a certified car inspection (CCI) of CN 302412 had been performed in Winnipeg, Manitoba, with no defects noted. Since a detached bell-crank bracket and bell crank would hang low and be easily identifiable to inspectors and operating employees, the bell-crank bracket and bell crank were probably in place at the time of the most recent CCI of CN 302412 and immediately before the accident.
Heavy corrosion on the fracture surfaces of the welds that secured the bell-crank bracket to the underside of the B-end sill of CN 302412 indicated that the cracks had likely been present (but undetected) for an extended period of time, including during the most recent CCI. However, a detailed inspection of the bell-crank bracket welds is not required during a CCI and any cracks in the welded securement would have been difficult to identify owing to the location of the welds. Regular pre-departure inspections, certified car inspections, and single-car air-brake tests did not detect the cracked bell-crank bracket welds prior to failure.
As specified in the Transport Canada (TC)-approved Railway Freight Car Inspection and Safety Rules, the TC-approved Railway Safety Appliance Standards Regulations, and the Association of American Railroads (AAR) Manual of Standards and Recommended Practices (MSRP) Standard S-2044, safety appliances must be secured to a car body using bolts or rivets. Welding is not permitted. While a loose bolt or rivet could be difficult to identify, a missing bolt or rivet would be readily identifiable during a visual inspection. In comparison, detecting cracks in welds requires a more detailed inspection. As this occurrence demonstrated, a weld crack can progress to failure before detection. For this reason, safety appliances are required to be secured with either bolts or rivets.
The securement of safety appliances to the car body is also inspected more frequently than is the securement of other appurtenances. For example, inspectors are instructed to observe safety appliances during a CCI to ensure they are properly secured, and to observe the securement of braking appliances during single-car air-brake tests. Since the bell-crank bracket and bell crank are not considered to be safety appliances, they are not required to be observed as often and inspectors are not instructed to specifically evaluate the bell-crank bracket securement.
Following the accident, the Canadian National Railway Company (CN) initiated a detailed inspection of its open-top hopper fleet and subsequently identified that 63 of 857 cars had a total of 71 defects, which included 5 bell-crank bracket defects. Since most of these cars had been subjected to various regular inspections with few defects noted, this demonstrates that the regular pre-departure inspections, CCIs, and single-car air-brake tests are not always sufficient to detect defects, prior to failure, that affect the safe operation of hand brakes.
The hand brake was rendered ineffective when the bell-crank bracket and the bell crank, which are not considered safety appliances, detached from the car body. If the securement of bell-crank brackets and bell cranks, which are critical to the safe operation of hand brakes, does not require the same mounting and inspection criteria as safety appliances, a defective bell crank can compromise hand-brake effectiveness, which increases the risk of accidents.
2.2.3 Egress from hand-brake end platform
At the time of the occurrence, employees would sometimes board moving equipment while switching. However, since 05 November 2018, CN has prohibited employees from boarding moving equipment, except when equipment is left unattended under the provisions of Canadian Rail Operating Rules (CROR) Rule 112 respecting securement;Footnote 79 in this instance, CN continues to expect its employees to apply a hand brake on moving equipment.
On CN 302412, the hand-brake end platform was positioned 90 inches above the ground, and the hand brake wheel was positioned even higher. Current standards limit the height of the hand-brake end platform to about 48 inches. Given that CN 302412 was constructed before 2015, there was no requirement to modify this car to meet current standards.
The foreman initiated the independent brake application to stop the assignment, and an emergency air-brake application occurred about 18 seconds later. The TSB re-enactment confirmed that 18 seconds provided sufficient time for a person to run from the foreman’s estimated position on the ground to the approaching rail car, climb onto the high-mounted end platform, and fully apply the hand brake. In this occurrence, the hand brake wheel had been turned beyond what was required to fully apply the hand brake, indicating that the foreman had at least 18 secondsFootnote 80 to run to CN 302412 and apply the hand brake. Since the assignment was already stopped on the MR-lead track, it is likely that the collision activated the emergency air-brake application.
The sooner a properly functioning hand brake is applied to a car, the sooner the car begins to decelerate—which, in an emergency situation, could provide more time for egress. When hand brakes and end platforms are mounted high on a car, the additional time it takes to climb the ladder to the platform delays the application of the hand brake and reduces the opportunity for egress during an emergency. Furthermore, the extra height of the end platform increases the potential for injury when dismounting. If freight cars with high-mounted hand brakes and end platforms remain in service, hand-brake operation during an emergency might be delayed and employee emergency egress made more difficult, which increases the risk of employee injury.
2.3 Kicking cars in Melville Yard
Judgment and experience must be relied upon when determining the location and speed at which to release the kicked cars. Kicking cars at too great a speed results in the cars coupling too hard to the cars in the intended track or running out the other end. Kicking cars at too slow a speed results in the cars either stalling before clearing the track or rolling back and fouling the track. It is not possible to predetermine and standardize the proper speed at which to kick cars, because each freight car is unique and environmental conditions are constantly changing.
Remote control locomotive system (RCLS) trainees at Melville Yard were instructed to set the speed selector to 10 mph when kicking cars and to visually estimate when the cars have reached an adequate speed at which to release the cars being kicked. The foreman had successfully been kicking cars with the speed selector set at 7 mph earlier in the shift at other locations in the yard, and did not modify her strategy when kicking cars up the grade on the MR-lead track. Testing performed following the accident demonstrated that the 3 cars would not have reached track MR13 from where they were released when kicked at 7 mph.
2.3.1 Switching plan
Both crew members were qualified for their positions and were described as competent, conscientious, and quick to learn. The foreman had sufficient railway experience to be comfortable with operations in the rail yard. However, the assignment foreman’s plan to kick the 3 open-top hopper cars loaded with ballast into track MR13 on an ascending grade was inadequate because:
- there was insufficient room at the east end of the track to receive all 3 cars, which measured about 130 feet in total length;
- the cars did not have sufficient momentum to reach track MR13, since 7 mph was too slow to kick the 3 cars up the ascending grade; and
- the movement was not monitored to ensure speed was adequate for the cars to reach their intended destination before the foreman began to make the next movement into track MR19.
2.4 Crew training and experience
During the 2nd week of RCLS training, CN provided 1 week of practical training operating RCLS-controlled locomotives. Trainers strove to ensure that all trainees received at least 8 hours of time operating the Beltpack.
While Beltpack training for qualified conductors is generally sufficient to operate the RCLS equipment, it would not necessarily provide the experience needed when performing tasks that rely upon judgment, such as kicking cars up a grade. Given the multiple variables involved, the development of the judgment needed to carry out these types of movements effectively and safely under a variety of conditions can only be gained through on-the-job experience after training has been completed.
At Melville Yard, it was common practice for the foreman to control all yard movements, even though both crew members are equipped with Beltpacks. This practice limited the amount of operating experience that helpers received, potentially affecting their progress toward becoming competent and safe RCLS-switching foremen. Moreover, the pairing of junior employees together for yard assignments meant that knowledge transfer through coaching was limited.
The occurrence foreman had started working for CN in September 2014, and had qualified as a conductor in February 2015 and as an RCLS operator in November 2015. After being laid off from CN in April 2016, she worked at Cando Rail Services, which did not conduct switching using Beltpacks. After returning to CN in March 2017, the foreman worked 22 yard shifts, 17 of which were as a helper. The occurrence shift was only her 5th yard shift while acting as a foreman and operating a Beltpack.
Although the foreman had about 3 years of railway experience working with 2 different companies, she had limited recent opportunity to serve as the foreman of a 2-person crew, and similarly, to operate a locomotive consist with a Beltpack. This experience might not have been adequate to develop the skills and judgment necessary to safely kick cars up a grade consistently. The foreman’s limited experience in operating an RCLS during switching operations likely contributed to the development of an inadequate plan and the attempt to kick the 3 cars at too slow a speed in an area of known ascending grade.
2.5 Crew communication
Safe rail operations require that all crew members have shared expectations of how movements will be carried out and a complete understanding of the associated hazards. Therefore, ongoing communication between crew members throughout a shift is of paramount importance.
Recognizing that communication is an important means of maintaining a safe working environment, CN included the requirement for communication as part of its conductor training. In addition, CN’s General Operating Instructions require job briefings to ensure that all work is understood between crew members. The job briefing includes, among other topics, track characteristics, such as track grade; specific switching movements are not discussed because the strategy for each move is not always known at the time of briefing. At Melville Yard, it was common practice to communicate the switching moves over the radio during the shift, and for a foreman to make an announcement just prior to kicking cars.
In this occurrence, although the foreman and helper held 2 job briefings, several elements of the plan were not effectively communicated and/or coordinated, as follows:
- Each switching move was not discussed during the job briefings or as the work progressed.
- The helper believed that the foreman would be shoving the 3 cars into track MR13 and was unaware that the foreman intended to kick the 3 cars into track MR13. Thus, the helper was positioned about 50 feet along the track, beside the location where the 3 cars were to be placed, and was not in a position to intervene when the 3 kicked cars began to roll back.
- The helper’s view of the MR-lead track was obstructed by cars standing in the adjacent track MR14, so the helper could not see the assignment.
- There was no radio communication or discussion prior to the cars being kicked, including how to handle the possibility of a rollback.
Given that the crew members’ communications were infrequent and did not fully detail how the work was to be performed, there was insufficient communication between the crew members, contributing to the inadequate plan.
Although both crew members had passed the conductor training course, which discussed the importance of communication, they were known to be reserved. Furthermore, they were relatively inexperienced in their roles and had only worked together on one previous occasion. The crew members’ reserve, inexperience in working together, and relative inexperience in their roles on the day of the accident likely contributed to their infrequent communication during their shift.
2.5.1 Crew resource management
Crew resource management (CRM) training in aviation and other industries has been found to help crews develop the skills to overcome communication issues and coordinate their activities more effectively. Although communication was assessed during conductor training, neither crew member had received formal CRM training.
While adherence to operating rules requires crews to communicate at various times, there is currently no regulatory requirement to include CRM training as a module for locomotive engineer (LE) and conductor qualification and re-qualification. Consequently, the adoption of CRM training in the rail industry has been sporadic and the approach differs between railways. In particular, CN does not provide LEs and conductors with formal rail CRM training. If crew members do not receive enhanced CRM training to develop skills in crew coordination and communication, there is an increased risk that inadequate crew communication will lead to unsafe operations.
2.6 Foreman’s attempt to stop the uncontrolled movement
During RCLS training at Melville Yard, it was emphasized that, when kicking cars in Melville Yard from the MR-lead track into tracks MR19 to MR10, the ascending track gradient in the area can be problematic. The guidance to crews was to be in a position to observe the cars and intervene by boarding them and applying hand brakes should they begin to roll back unexpectedly.
When faced with a cut of cars rolling back on the MR-lead track, the foreman ran toward the uncontrolled movement, boarded the lead car—which was equipped with a high-mounted hand brake—and attempted to stop the movement by applying the hand brake. Due to the slow speed of the cars, the foreman likely believed that the cars could be stopped with the hand brake. While other options were available, the underlying reasons for this split-second decision will never be fully understood.
2.7 Pairing of inexperienced operators
The U.S. Federal Railroad Administration (FRA) conducted a study on RCLS operations. Although the study was primarily focused on the practices of U.S. railroads (with 1 of the focus groups including Canadian railways), the analysis and results are applicable to the North American railway industry.
The report highlighted the concern that new hires trained as RCLS operators need time to develop knowledge and skills in railway operations. The report also identified the risks of pairing inexperienced crew members together when operating RCLS. The report further highlighted that not having training for a specific movement or area of the yard was a contributor to previous accidents involving RCLS operations.
Since 2007, the TSB has completed 6 investigations (including this occurrence) that highlighted the risks associated with conductors with low levels of experience being paired together to carry out yard assignments (Appendix C). The TSB determined that the experience level of the conductors contributed to these occurrences through increased likelihood of errors, and insufficient knowledge to make effective decisions with respect to planning and train handling. Further, the TSB determined that the practice of pairing junior employees together for yard assignments meant that the coaching and mentoring required to develop the effective judgment needed for train handling were not being provided.
There is no company or regulatory requirement outlining the time or experience required before a conductor assumes the role of yard foreman. However, before an employee can be qualified as a foreman, the employee must demonstrate the competencies required to perform such work. At CN, the member of the crew with the most seniority at the railway would typically be assigned the role of foreman, regardless of the employee’s experience at the task. Because CN’s scheduling system assigns operating employees to yard positions based on seniority, it is possible for yard foremen to have limited operational and RCLS experience. If the role of yard foreman has no requirements related to their experience with the tasks involved, the scheduling system used to fill the positions can result in inexperienced employees being put in charge of unfamiliar tasks, increasing the risk of error.
2.8 Regulatory oversight of railway operating employee qualifications and training
The Railway Employee Qualification Standards Regulations governing railway operating employees identify the subjects in which each candidate in 4 separate occupational categories is required to be trained. However, because the regulations have not been updated in more than 30 years, the regulations do not reflect some newer aspects of the railway operating environment. RCLS is one such subject. Consequently, required training in RCLS is not a part of any occupational category.
The Railway Safety Act review panel examined the training and qualification issue in its report entitled Stronger Ties: A Shared Commitment to Railway Safety – Review of the Railway Safety Act, which was released in 2007. The panel examined the Railway Employee Qualification Standards Regulations as they related to operating employee qualification standards, graduated qualification, training, and regulatory oversight. The review panel’s report identified the fact that the regulatory framework for railway employee qualification has not kept pace to reflect the significant changes in the railway operating environment.
In a previous TSB investigation (R16T0111), deficiencies in the current Railway Employee Qualification Standards Regulations were highlighted. In that investigation, the Board noted that TC’s 2017–18 Departmental Plan highlighted its intention to update the Railway Employee Qualification Standards Regulations, but there was little progress at that time. As a result, the Board recommended that TC update the regulations to address the existing gaps for railway employees in safety-critical positions related to training, qualification, and re-qualification standards, and regulatory oversight.
The training and qualification issue was again examined by the 2018 Railway Safety Act review panel. Its report entitled Enhancing Rail Safety in Canada: Working Together for Safer Communities included the following conclusion:
- The Review is satisfied and encouraged by Transport Canada’s current efforts to update and broaden its approach to the railway employee qualification and training framework, with a view to revising/replacing the existing regulations. This is an important undertaking, given the number of railway industry changes in the areas of new technology, increased staff turnover, and associated new hires.Footnote 81
However, the existing regulations have not yet been replaced. If the Railway Employee Qualification Standards Regulations are not updated, effective regulatory oversight and enforcement of safety-critical positions will be compromised, increasing the risk of unsafe train operations.
2.9 Safety management systems
In addition to the Railway Employee Qualification Standards Regulations, sections 25 to 27 of the Railway Safety Management System Regulations require the railway to have a process for managing knowledge that includes training and qualifications for the positions in the railway company that perform duties essential to safe railway operations. With regard to managing knowledge, CN had a detailed list of essential duties for LEs, conductors, and RCLS operators. CN also listed the skills and qualifications required to perform essential duties and a process for operating employees. The listed skills and qualifications for RCLS operators and conductors did not include train handling and locomotive operations. Further, there were no minimum experience requirements for work in the capacity of yard foreman and RCLS operator.
CN’s Partners in Prevention program recognizes the need for open, effective communication to drive safety improvements rather than relying on a punitive system to encourage safe behaviours. This program is a positive step toward developing a company SMS that perceives incidents, including those involving human error, as learning opportunities that in turn help develop a more resilient safety culture.
Effective safety management also requires the identification of systemic issues to assist in the prevention of accidents and the reporting of contraventions and safety hazards by employees without fear of reprisal. For this occurrence, the area in the yard where the accident happened (MR-lead track) was an area where uncontrolled movements were known to occur. A review of the TSB Railway Occurrence Database (RODS) determined that this occurrence was the 12th uncontrolled movement in Melville Yard over the previous 10 years. Of these 12 uncontrolled movements, 8 occurred in the MR-lead area, including 3 rollbacks and 5 movements related to inadequate securement. These data only included incidents that resulted in an adverse consequence and were reported to the TSB.
2.9.1 Canadian National Railway Company close-call reporting
The rail industry’s long-standing history of punitive processes used to address employee infractions and violations may be an impediment to gathering accurate self-reported close-call data.
However, some railway companies have begun to implement close-call reporting. For example, VIA Rail Canada Inc. (VIA Rail) crews are encouraged to report near misses at crossings in order to help identify problem roadway crossings. VIA Rail crews are also encouraged to self-report instances of close calls or rule violations with the understanding that there will be no discipline, or discipline will be reduced, if the crew self-identifies.
In 2013, CN established an independent close-call reporting hotline for employees called PREVENT, which was managed through St. Mary’s University, in Halifax, Nova Scotia. Employees were encouraged to call in near misses and close calls. St. Mary’s University edited the data to ensure that the reports remained confidential. However, the results were limited and the program ceased operation in 2017.
Under CN’s SMS Procedure and Policy for Reporting Contraventions or Safety Hazards, employees are instructed to report all safety hazards and concerns to local management. Employees who want to report a contravention or safety hazard without fear of reprisal are instructed to contact the CN Ombudsman’s office. From 2009 to 2018 inclusive, the ombudsman’s office received 147 confidential reports related to safety, which equates to approximately 1 report per month.
While some safety issues have been reported to the CN Ombudsman’s office, this process has not typically been advertised as a close-call reporting system. This investigation has identified that, while many employees had experienced rollbacks on the MR-lead track, they were unlikely to report to the company those that did not result in a collision, a derailment, or damage to either track or rolling stock, because they could potentially be subject to disciplinary action. Therefore, the total number of uncontrolled movements in this area, including those that did not result in damage, may be higher yet remain undetected. If a railway’s SMS does not include comprehensive close-call reporting of systemic operational issues that do not result in adverse consequences, effective mitigation strategies will not be implemented, which increases the risk that similar or more serious accidents will continue to occur.
2.10 Uncontrolled movements in Melville Yard
As a result of the TSB investigation into the Lac Mégantic accident,Footnote 82 the Board recommended that TC require Canadian railways to put in place additional physical defences to prevent runaway equipment (TSB Recommendation R14-04). In response, TC implemented a number of initiatives, including strengthening securement requirements in Canadian Rail Operating Rules (CROR) Rule 112 and introducing a comprehensive oversight plan for the new rule. Although the Board was encouraged by the TC initiatives, it noted that current defences do not seem sufficient to reduce the number of uncontrolled movements and improve safety.
In a subsequent TSB railway investigation report,Footnote 83 which involved an uncontrolled movement while switching without air, the Board issued a safety concern stating that the current defences are not sufficient to reduce the number of uncontrolled movements and improve safety.
Although training and experience can reduce errors when switching cars, including kicking cars when switching without air, they cannot be relied upon to eliminate them. The history of uncontrolled movements on the MR-lead track demonstrates that the ascending grade in this area could be particularly challenging. CN was aware of this and had identified the primary causes of the uncontrolled movements on the MR-lead track as being inadequate securement and operator errors. While CN’s local corrective measures focused on individual employee education, clarification of instructions, and increased monitoring, these corrective measures did not fully address the challenges associated with switching on the ascending grade of the MR-lead track.
2.11 Unplanned/uncontrolled movement statistics
Between 2009 and 2018, 562 unplanned/uncontrolled movements occurred, and the trend during the 10-year period was on an upward trajectory. This trend indicated an additional 1.67 occurrences each year, with 86% of the overall increase associated with switching without air. During that period, there were 185 occurrences involving switching without air; 70 (38%) occurred as a result of rollbacks and 56 (30%) involved dangerous goods. The major outcomes of these occurrences were collisions (134, or 72%) and derailments (76, or 41%). Two (1%), including this occurrence, involved an employee fatality.
While switching without air is routine and occurs every day in the rail industry, the practice does have some inherent risks that can result in serious consequences. If effective strategies are not taken to improve safety while switching without air, uncontrolled movements will continue to occur, increasing the risk of adverse outcomes. Despite safety action taken by TC and the railway industry, the desired outcome of significantly reducing the number of uncontrolled movements has not yet been achieved.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The accident occurred when 3 open-top hopper cars loaded with ballast were kicked up an ascending grade on the MR-lead track, stalled, rolled back, and collided with the lead car of the assignment, empty car PLCX 21492, which was foul of the lead track.
- While attempting to stop the uncontrolled cars by applying the hand brake on CN 302412, the foreman became pinned between PLCX 21492 and CN 302412, receiving fatal injuries.
- When the foreman applied the hand brake, the welds securing the bell-crank bracket to the underside of the B-end sill of CN 302412 failed, and the bell crank and the bracket separated from the car, rendering the hand brake ineffective.
- Because the braking efficiency of the hand brake was compromised, the uncontrolled movement did not stop or slow, which reduced the opportunity and time for the foreman to safely egress.
- Regular pre-departure inspections, certified car inspections (CCI), and single-car air-brake tests did not detect the cracked bell-crank bracket welds prior to failure.
- The assignment foreman’s plan to kick the 3 open-top hopper cars loaded with ballast into track MR13 on an ascending grade was inadequate because it did not take into consideration the amount of room required to receive all 3 cars, the momentum required for the cars to reach the track, and the need to monitor the movement to ensure that the speed was adequate for the cars to reach their intended destination.
- The foreman’s limited experience in operating a remote-controlled locomotive system during switching operations likely contributed to the development of an inadequate plan and the attempt to kick the 3 cars at too slow a speed in an area of known ascending grade.
- There was insufficient communication between the crew members, contributing to the inadequate plan.
- The crew members’ reserve, inexperience in working together, and relative inexperience in their roles on the day of the accident likely contributed to their infrequent communication during their shift.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If the securement of bell-crank brackets and bell cranks, which are critical to the safe operation of hand brakes, does not require the same mounting and inspection criteria as safety appliances, a defective bell crank can compromise hand-brake effectiveness, which increases the risk of accidents.
- If freight cars with high-mounted hand brakes and end platforms remain in service, hand-brake operation during an emergency might be delayed and employee emergency egress made more difficult, which increases the risk of employee injury.
- If crew members do not receive enhanced crew resource management training to develop skills in crew coordination and communication, there is an increased risk that inadequate crew communication will lead to unsafe operations.
- If the role of yard foreman has no requirements related to their experience with the tasks involved, the scheduling system used to fill the positions can result in inexperienced employees being put in charge of unfamiliar tasks, increasing the risk of error.
- If the Railway Employee Qualification Standards Regulations are not updated, effective regulatory oversight and enforcement of safety-critical positions will be compromised, increasing the risk of unsafe train operations.
- If a railway’s safety management system does not include comprehensive close-call reporting of systemic operational issues that do not result in adverse consequences, effective mitigation strategies will not be implemented, which increases the risk that similar or more serious accidents will continue to occur.
- If effective strategies are not taken to improve safety while switching without air, uncontrolled movements will continue to occur, increasing the risk of adverse outcomes.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- Prior to the collision, the hand brake wheel on CN 302412 had been turned beyond what was required to fully apply the hand brake.
- Once the hand brake was fully applied, a fully effective hand brake on car CN 302412 could have stopped the uncontrolled movement within the available distance.
- Since a detached bell-crank bracket and bell crank would hang low and be easily identifiable to inspectors and operating employees, the bell-crank bracket and bell crank were probably in place at the time of the most recent certified car inspection of CN 302412 and immediately before the accident.
- Heavy corrosion on the fracture surfaces of the welds that secured the bell-crank bracket to the underside of the B-end sill of CN 302412 indicated that the cracks had likely been present (but undetected) for an extended period of time, including during the most recent certified car inspection.
- A detailed inspection of the bell-crank bracket welds is not required during a certified car inspection and any cracks in the welded securement would have been difficult to identify due to the location of the welds.
- The Canadian National Railway Company initiated a detailed inspection of its open-top hopper fleet and subsequently identified that 63 of 857 cars had a total of 71 defects, which included 5 bell-crank bracket defects.
- Since the assignment was already stopped on the MR-lead track, it is likely that the collision activated the emergency air-brake application.
- While the Canadian National Railway Company’s local corrective measures focused on individual employee education, clarification of instructions, and increased monitoring, these corrective measures did not fully address the challenges associated with switching on the ascending grade of the MR-lead track.
- Despite safety action taken by Transport Canada and the railway industry, the desired outcome of significantly reducing the number of uncontrolled movements has not yet been achieved.
4.0 Safety action
4.1 Safety action taken
4.1.1 Canadian National Railway Company
Following the accident, several local notices and special instructions were issued identifying locations where the kicking of cars uphill was forbidden. On 01 February 2018, the Canadian National Railway Company (CN) issued System Operating Bulletin No. 001. The bulletin stated that, “[t]o prevent the possibility of unintentional rollbacks while switching, even if planning on riding the equipment to rest,” the following statement would be added to section 8.4.12 of the CN General Operating Instructions (GOI): “kicking or performing a running switch uphill is prohibited.”
With regard to protecting the point of movement by remote control locomotive system (RCLS) crews, on 01 May 2018, CN added the following to section 6 of its GOI:
6.5 OPERATING AND SWITCHING REQUIREMENT
6.5.1 Operating Restrictions – Replaced by the following:
- Assignments with 2 crew members must have 2 operative OCUs [operator control units] at the beginning of their shift;
- Operative OCU’s must be worn at all times. The employee on the point of movement is to be in control, by use of ‘pitch and catch’ function (Not applicable when one operator has a defective OCU);
- when pulling or shoving by more than 20 car lengths or,
- when the movement may be required to stop for switches, signals, derails, end of track, red flags.
- RCO [remote control operator] must be able to see and monitor the movement at all times. The primary focus should be controlling the movement; Distractions must be avoided [….]Footnote 84
Following the accident, CN reviewed the way switching was being performed at Melville Yard. As a result, CN identified areas where track reconfiguration and changes to the track gradient would significantly reduce the likelihood of a rollback and uncontrolled movement. Switching was moved to the west end of the yard, where the above modifications have been made.
4.2 Safety action required
4.2.1 Reducing the frequency and associated risks of uncontrolled movements while switching without air
In this occurrence, a foreman was controlling a yard assignment using an RCLS while switching without air in Melville Yard. During switching operations, the foreman became pinned between the assignment and the lead car of an uncontrolled movement while attempting to stop the movement by applying a hand brake. As a result, the foreman received fatal injuries.
Uncontrolled movements generally fall into 1 of 3 broad causal categories: loss of control, switching without air, and securement. Since 2016, the TSB has completed 3 investigations,Footnote 85 including this one, involving uncontrolled movements that occurred in yards while switching without air.
Switching without air occurs when a movement is switching with the use of the locomotive independent brakes, only with no air brakes available on the cars being switched or kicked. The vast majority of these incidents occur in yards.
Similar to this occurrence, TSB occurrence R16W0074 involved relatively inexperienced operators who were conducting switching operations without air in Canadian Pacific Railway (CP)’s Sutherland Yard in Saskatoon, Saskatchewan. The investigation determined that, despite Transport Canada (TC) and industry initiatives, the desired outcome of significantly reducing the number of uncontrolled movements had not yet been achieved. Consequently, the Board was concerned that the current defences were not sufficient to reduce the number of uncontrolled movements and improve safety.
Between 2009 and 2018, 562 unplanned/uncontrolled movements occurred. There has been an upward trend during this 10-year period. The average increase per year for all categories was 1.67 occurrences, with 86% of the overall increase associated with switching without air. Of the 185 occurrences involving switching without air, 70 (38%) occurred as a result of rollbacks and 56 (30%) involved dangerous goods. The major outcomes of these occurrences were collisions (134, or 72%) and derailments (76, or 41%). Two of the occurrences (1%), including this occurrence, involved an employee fatality.
While switching without air is routine and occurs every day in the railway industry, the practice has some inherent risks that can result in serious consequences. If effective strategies are not taken to improve safety while switching without air, uncontrolled movements will continue to occur, increasing the risk and severity of adverse outcomes.
The railway industry is responsible for having rules, instructions, procedures, and processes in place to safely manage operations. Railway employees who are directly involved in these operations have the greatest knowledge of how the work actually gets done and are the most affected when accidents occur. However, the regulator also has a responsibility to have adequate regulations, rules, and enforcement in place in order to provide effective regulatory oversight to ensure safe operations.
Safety action taken by TC and the railway industry to date has focused on securement practices. However, the desired outcome of significantly reducing the number of uncontrolled movements has not yet been achieved.
The underlying causes of uncontrolled movements that occur while switching without air can vary greatly. Consequently, developing a comprehensive strategy to deal effectively with all of the underlying factors and associated risks in order to reduce the number of such uncontrolled movements is proving to be difficult. Therefore, the Board recommends that
The Department of Transport work with the railway industry and its labour representatives to identify the underlying causes of uncontrolled movements that occur while switching without air, and develop and implement strategies and/or regulatory requirements to reduce their frequency.
TSB Recommendation R20-01
4.3 Safety concern
4.3.1 Pairing of inexperienced remote control locomotive system operators
In the railway industry, conductors are assigned the task of being RCLS operators, particularly in rail yards across the country. Conductors are generally unionized positions that are governed by collective agreements between the employer and the union. In most cases, local yard assignments are posted for bidding each week. After the employees submit their bids, the positions are awarded based on seniority in accordance with the collective agreement.
Some of the posted positions are favoured owing to the rate of pay, days off, and hours of work. Typically, the evening shifts and the night shifts are considered the least desirable, and yard positions in particular are normally regarded as the least desirable because the pay rates for these positions are the lowest. If no bids are received for a specific position, the position is awarded to the employee with the least seniority.
As extensive employee turnover has been occurring in the railway industry in the past few years, it is not unusual for the 2 most junior, and least experienced, employees at a terminal to be working together in yards, particularly during the evening and night shifts. The pairing of inexperienced crew members is not uncommon in the Canadian railway industry.
Since 2007, the TSB has completed 6 investigations (including this occurrence) that highlight the risks associated when conductors with low levels of experience are paired together to carry out yard assignments (Appendix C). The TSB determined that the relative inexperience of the RCLS operators (conductors) contributed to these occurrences through insufficient knowledge to make effective decisions with respect to planning and train handling. Further, the TSB determined that the practice of pairing junior employees together for yard assignments meant that the coaching and mentoring needed to develop effective judgment for train handling were not being provided.
While an operating employee must demonstrate the competencies required to perform work as a qualified foreman, there is no company or regulatory requirement outlining the time or experience required before a conductor assumes the role of yard foreman. These roles are tied to a collective agreement for unionized staff. Consequently, the crew member with more seniority at the railway would typically be assigned the role of foreman, regardless of the employee’s experience with the task.
Furthermore, because railway scheduling systems will typically assign operating employees to yard positions based on seniority, it is possible for yard foremen to have limited operational and RCLS experience. If the role of yard foreman has no requirements relating to experience with the tasks involved, the scheduling system used to fill the positions can result in inexperienced employees being put in charge of unfamiliar tasks, which increases the risk of errors and accidents.
Given the ongoing employee turnover in the railway industry and the potential adverse outcomes when inexperienced RCLS operators are paired together working in yards, the Board is concerned that, without additional mitigation, inexperienced RCLS operators will continue to be paired together in yards with a commensurate risk of ongoing adverse outcomes.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Uncontrolled movements in Melville Yard in the 10 years preceding the occurrence
| Occurrence number | Date | Summary | Cause |
|---|---|---|---|
| R17W0047 | 2017-02-26 | Canadian National Railway Company (CN) Melville Beltpack assignment set off loaded rail car COER 800982 (load of iron ore) on track MR19. The car soon after rolled away and side-swiped Beltpack locomotive CN 7258 on the lead track. No injuries were reported. There was no derailment. No dangerous goods were involved. The car and locomotive sustained damage. | Securement |
| R14W0274 | 2014-11-02 | While switching, CN Melville Beltpack yard assignment YMYS60 released 2 cars onto track MR13. While standing on the lead, the cars returned from track MR13, resulting in car IC 799619 (empty covered hopper car) colliding with slave unit CN 268. No injuries were reported. There was no damage and no derailment. | Rollback |
| R14W0264 | 2014-10-04 | During normal switching operations, CN Beltpack yard assignment YMYS60 moved 20 cars onto the east lead track to set off 1 car on MR13. As the assignment returned to the lead track, the 20 cars had rolled back about 100 feet, resulting in a collision with the yard assignment. No injuries were reported. No dangerous goods were involved. Safety appliances on 2 of the cars sustained damage. | Securement |
| R14W0175 | 2014-07-20 | During switching operations from east lead MX01, 4 cars loaded with salt rolled back from the lead while the crew (CN 0830 yard assignment) was releasing 3 additional cars onto track MA10. Car NMIX 86030 collided with car NMIX 9508, derailing both cars and 2 others, NMIX 9115 and NMIX 172503, all upright. No injuries were reported. No dangerous goods were involved. Approximately 200 feet of track sustained damage. | Rollback |
| R14W0170 | 2014-07-12 | While CN 1545 extra yard assignment was switching at Melville, car GATX 57254 (residue car last containing liquefied petroleum gas) rolled eastward on track MR14 and derailed when it sideswiped car PROX 31866 (residue car last containing liquefied petroleum gas) on the east lead. No injuries were reported. Both cars sustained damage. | Rollback |
| R13W0342 | 2013-07-06 | After pulling cars from rip track MR23 in Melville Yard, the CN yard crew on the 1530 yard assignment reported that car CN 383183, which had been left in the track, rolled uncontrolled and derailed over the derail. No injuries were reported. No dangerous goods were involved. | Securement |
| R13W0340 | 2013-04-23 | After the 1530 yard assignment set off a cut of cars in track MR13 in Melville Yard, it was reported that the cars began to roll uncontrolled and contacted a car on the lead track. As a result of the collision, 1 covered hopper car sustained damage. No injuries were reported. No dangerous goods were involved. | Securement |
| R13W0171 | 2013-07-01 | While switching in Melville Yard, CN yard assignment YMY-605-30 set off a cut of cars onto the lead track before entering track MR16. It was reported that the cars on the lead track began to roll uncontrolled and side-contacted the assignment. No injuries were reported. No dangerous goods were involved. As a result of the collision, 2 cars sustained damage. | Securement |
| R10W0257 | 2010-11-10 | CN 1400 yard assignment, while pulling cars from track MA10 in Melville Yard, was struck by a cut of cars rolling uncontrolled from track MR05. As a result of the collision, 1 car derailed. No injuries were reported. No dangerous goods were involved. | Securement |
| R09W0278 | 2009-11-22 | CN 0600 east yard assignment set off a cut of 2 cars into track MR14 in Melville Yard and then proceeded into track MR16. It was reported that the cars in track MR14 began to roll uncontrolled. The cars side-contacted and derailed the flat car being shoved into track MR16. No injuries were reported. No dangerous goods were involved. | Securement |
| R08W0086 | 2008-04-22 | CN 1400 yard assignment reported being struck by car CNLX 10262 while pulling 2 cars from track MA05 in Melville Yard. Car CNLX 10262 derailed and the other 2 cars sustained damage. The 1400 yard assignment had just placed car CNLX 10262 in track MA10 when it ran uncontrolled out of the track, leading to the collision. No injuries were reported. | Securement |
Appendix B – Railway Employee Qualification Standards Regulations
The Railway Employee Qualification Standards Regulations state, in part:
General
- A railway company shall provide employee training necessary for the purposes of these Regulations.
(1) No railway company shall permit any employee to work as a locomotive engineer, transfer hostler, conductor, or yard foreman unless the employee
(a) has qualified for that occupational category in accordance with section 14; and
(b) in the case of a locomotive engineer or transfer hostler, has received a passing mark for on-job training in that occupational category. […]
- A railway company shall provide to its locomotive engineer candidates and transfer hostler candidates sufficient on-job training in respect of the required subjects to enable them to demonstrate to instructors and examiners that they are competent to perform their required duties.
- No examiner shall issue a passing mark for on-job training to a locomotive engineer candidate or transfer hostler candidate unless the examiner
- is satisfied that the candidate is competent to perform his required duties by
- obtaining an evaluation of the candidate’s competency from the locomotive engineer or transfer hostler with whom the candidate has made student on-job training trips, and
- assessing the candidate’s competency in actual locomotive or train operation, or both, depending on the requirements of the occupational category for which the candidate is being examined; and
- has completed, signed and placed on the candidate’s personnel file a document indicating that the candidate has passed the on-job training.
- An examiner shall determine the overall mark for a candidate based on written or oral classroom examinations, or both, dealing with the required subjects.
- An employee undergoing on-job training in order to qualify as a locomotive engineer or transfer hostler may perform the duties of the occupational category for which he is a candidate under the direction of an on-job training instructor for the duration of the employee’s training period.
(1) A railway company shall, at intervals of not more than three years, have each employee in an occupational category re-examined on the required subjects.
(2) The overall pass mark for re-examination is 80 per cent. […]
(1) Within 90 days after the coming into force of these Regulations, a railway company shall file with the Committee two copies of each type of classroom examination and two copies of a detailed description of each method of assessing on-job competence used by the company.
(2) A railway company shall notify the Committee of a change to a type of classroom examination format or method of assessing on-job competence within 90 days after implementing the change. […]
Qualification Standards for Candidates
(1) The subjects required for a person to qualify for an occupational category are the subjects listed in those items of the schedule marked with an “X” under the heading that corresponds to the occupational category, excluding those subjects or portions of subjects dealing with equipment that is not used by the railway company that employs the person.
(2) No railway company shall qualify a person for an occupational category unless the person obtains an overall mark of at least 80 per cent in the required subjects.
Qualification Standards for On-job Training Instructors
No railway company shall qualify a person as an on-job training instructor for the occupational category of locomotive engineer unless the person
(a) meets the qualification requirements for a locomotive engineer with an overall mark of at least 90 percent; and
(b) completes not less than two years service as a locomotive engineer, including at least three months service in the area where the locomotive engineer is to give the on-job training.
No railway company shall qualify a person as an on-job training instructor for the occupational category of transfer hostler unless the person
(a) meets the qualification requirements for a transfer hostler with an overall mark of at least 90 per cent; and
(b) completes not less than one year of service as a transfer hostler, including at least three months service in the area where the transfer hostler is to give the on-job training.
Qualification Standards for Classroom Training Instructors
- No railway company shall qualify as a classroom training instructor for a required subject a person who has not obtained a mark of at least 90 per cent in a written examination on that subject.
Qualification Standards for Examiners
- An employee or officer of a railway company who is an on-job training instructor or a classroom training instructor is qualified to act as an examiner on the subjects on which the employee or officer is qualified to give instruction.
Training Programs and Consultation
(1) A railway company shall establish employee training programs for each occupational category.
(2) A railway company shall establish and modify its employee training programs in consultation with the trade unions representing its employees in the occupational categories.
(3) Within 90 days after the coming into force of these Regulations, a railway company shall file with the Committee a description of all employee training programs relating to each occupational category.
(4) Within 90 days after any change is made to an employee training program required by subsection (1), a railway company shall file with the Committee a description of the change.
Reporting
(1) For each calendar year a railway company shall submit to the Committee, not later than March 31 of the following year, a comprehensive report on its employee training programs.
(2) A report referred to in subsection (1) shall specify
- the total number of employees in each occupational category;
- the total number of employees who received training in each occupational category;
- the number of employees who received training and met the training requirements for each category and the number who failed to meet the training requirements; and
- any new or improved techniques or devices adopted in the company’s employee training programs.
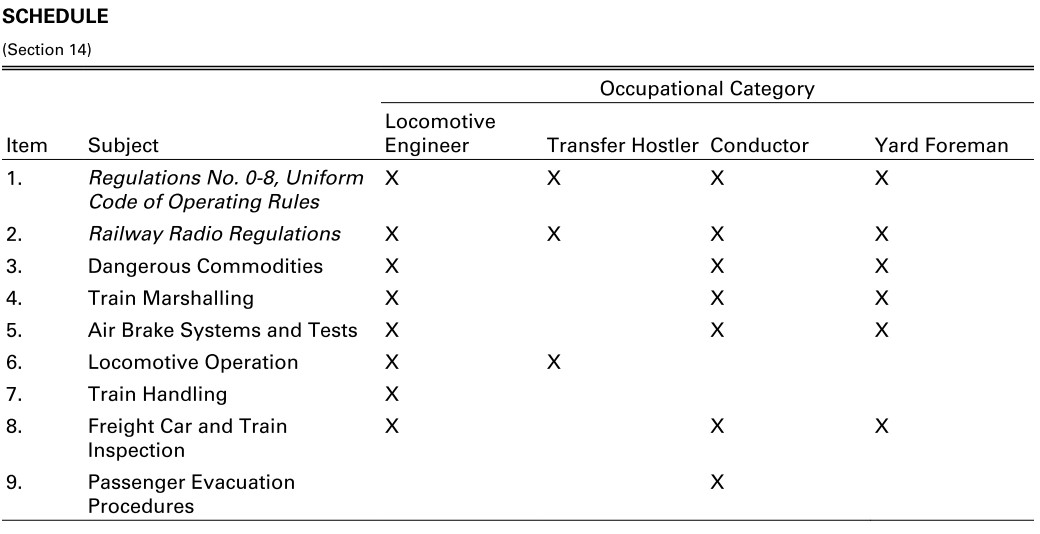
Appendix C – Other TSB investigations involving training or experience while switching using remote control locomotive systems
R16T0111 – On 17 June 2016, the Canadian National Railway Company (CN) remote control locomotive system (RCLS) 2100 west industrial yard assignment was performing switching operations at the south end of CN’s MacMillan Yard, located in Vaughan, Ontario. The assignment was in the process of pulling 72 loaded cars and 2 empty cars southward from the yard onto the York 3 main track to clear the switch at the south end of the Halton outbound track to gain access to the west industrial lead track (W100) switch. While attempting to stop in preparation for reversing into track W100 to continue switching for customers, the yard helper lost control of the assignment. The assignment rolled uncontrolled for about 3 miles, reaching speeds of up to 30 mph before stopping on its own at about Mile 21.1 of the York Subdivision. There were no injuries. There was no release of dangerous goods and no derailment.
The investigation determined that:
- The assignment crew did not have sufficient operational experience to safely perform the tasks of the west industrial yard assignment at MacMillan Yard.
- Conductors receive little training in locomotive operation and train handling, and the current Railway Employee Qualification Standards Regulations do not require such training.
- While the assignment crew was aware of the assignment’s length and weight, they lacked the knowledge to fully understand the effect that the assignment’s length and weight had on train handling while descending a 0.70% grade with only locomotive independent brakes available to control the assignment.
R16W0074 – On 27 March 2016, while switching in Sutherland Yard in Saskatoon, Saskatchewan, Canadian Pacific Railway (CP) 2300 RCLS training yard assignment was shoving a cut of cars into track F6. As the assignment was brought to a stop, empty covered hopper car EFCX 604991 uncoupled from the train, unnoticed by the crew. The car rolled uncontrolled through the yard and onto the main track within cautionary limits of the Sutherland Subdivision. The car travelled about 1 mile and over 2 public automated crossings before coming to a stop on its own. There were no injuries and no derailment. No dangerous goods were involved.
The investigation determined that:
- The combination of learning the additional tasks associated with RCLS operations and managing the point protection zone, combined with the relative inexperience of the yard crew, contributed to the slip of attention relating to the coupler.
R07T0270 – On 17 September 2007, while pulling south on the pullback track with a consist of 67 loaded and 30 empty cars, weighing about 9054 tons, CN yard assignment YWCS60-17 side-collided with the tail end of CN freight train M33931-17. The freight train was departing MacMillan Yard in Vaughan, Ontario, near Toronto, Ontario, at 15 mph on the Halton outbound track. Two locomotives and 2 cars of the yard assignment derailed. On the freight train, 6 cars derailed and/or sustained damage, including 2 special dangerous goods tank cars containing chlorine (UN1017). Approximately 3785 litres of diesel fuel (UN1202) leaked from the derailed locomotives. There were no injuries.
The investigation determined that:
- Although CN had recently qualified the helper to operate RCLS switching assignments, neither his training nor experience were adequate for switching long, heavy cuts of cars on tracks with descending grades.
- While conductor trainees receive basic instruction and testing in handling yard movements as part of their RCLS training, they do not receive specific instruction or practical experience on the effects of tonnage, length, marshalling, or topography on braking distances. In the absence of such training, newly trained personnel might not be adequately qualified to safely operate yard movements at all times.
- The qualifying test to certify conductors in RCLS yard operations was not sufficiently rigorous to evaluate conductor trainee skills under work conditions. Consequently, trainees without the requisite skill or experience were being placed in active service without restrictions.
R07V0213 – On 04 August 2007, a CN RCLS assignment was pulling 53 loaded cars from track PA02 at the north end of Prince George South Yard, in Prince George, British Columbia. While attempting to clear the switch to access the classification tracks, the movement ran away northbound, striking a CN freight train which was entering the north end of the yard. The RCLS assignment struck a tank car loaded with gasoline, derailing it as well as the next tank car ahead, also loaded with gasoline. The tank cars released product and a fire ensued.
Two locomotives, a slug unit, and a loaded centrebeam flat car in the yard assignment derailed and, along with the 2 tank cars from the other train, were destroyed in the subsequent fire. Approximately 172 600 litres of fuel (1600 litres of diesel and 171 000 litres of gasoline) were spilled. Most of the released fuel was consumed by the fire. There were no injuries.
The investigation determined that:
- Although considered qualified from a regulatory perspective for their respective duties, the management employees operating the RCLS switching assignment were inadequately trained and had no experience switching long, heavy cuts of cars on the pullback track descending grade.
- The practice of temporarily assigning management employees to do the work of experienced operating employees might increase the risk of accidents.
R07W0042 – On 13 February 2007, a CN hump yard assignment was performing switching operations at Symington Yard in Winnipeg, Manitoba. While travelling westward at approximately 6 mph on track ER-08, the hump yard assignment sideswiped a CN train, which was outbound on track ER-04. Four cars from the hump assignment derailed. A total of 9 cars were damaged. No dangerous goods were involved and there were no injuries.
The investigation determined that:
- Insufficient training, combined with the operator’s limited practical experience, likely contributed to the omission of confirming the direction of travel immediately after initiating the RCLS command.
Appendix D – TSB investigations involving uncontrolled movements
| Occurrence number | Date | Description | Location | Cause |
|---|---|---|---|---|
| R18Q0046 | 2018-05-01 | Uncontrolled movement and derailment of rolling stock on non-main track, Quebec North Shore and Labrador Railway (QNS&L), cut of cars, Sept-Îles Yard |
Sept-Îles, Quebec | Switching without air |
| R17V0096 | 2017-04-20 | Non-main-track uncontrolled movement, collision, and derailment, Englewood Railway, Western Forest Products Inc., cut of cars | Woss, British Columbia | Switching without air |
| R16W0242 | 2016-11-29 | Uncontrolled movement, collision, and derailment, Canadian Pacific Railway (CP), Ballast train BAL-27 and Freight train 293-28, Mile 138.70, Weyburn Subdivision | Estevan, Saskatchewan | Loss of control |
| R16T0111 | 2016-06-17 | Uncontrolled movement of railway equipment, Canadian National Railway Company (CN), remote control locomotive system (RCLS) 2100 west industrial yard assignment, Mile 23.9, York Subdivision, MacMillan Yard | Vaughan, Ontario | Loss of control |
| R16W0074 | 2016-03-27 | Uncontrolled movement of railway equipment, CP, 2300 RCLS training yard assignment, Mile 109.7, Sutherland Subdivision | Saskatoon, Saskatchewan | Switching without air |
| R16W0059 | 2016-03-01 | Uncontrolled movement of railway equipment, Cando Rail Services, 2200 Co‑op Refinery Complex assignment, Mile 91.10, Quappelle Subdivision | Regina, Saskatchewan | Securement |
| R15D0103 | 2015-10-29 | Runaway and derailment of cars on non-main track, CP, Stored cut of cars, Mile 2.24, Outremont Spur | Montréal, Quebec | Securement |
| R15T0173 | 2015-07-29 | Non-main-track runaway, collision, and derailment, CN, Cut of cars and train A42241‑29, Mile 0.0, Halton Subdivision | Concord, Ontario | Switching without air |
| R13D0054 | 2013-07-06 | Runaway and main-track derailment, Montreal, Maine & Atlantic Railway, Freight train MMA-002, Mile 0.23, Sherbrooke Subdivision | Lac-Mégantic, Quebec | Securement |
| R12E0004 | 2012-01-18 | Main-track collision, CN, runaway rolling stock and train A45951-16, Mile 44.5, Grande Cache Subdivision | Hanlon, Alberta | Securement |
| R11Q0056 | 2011-12-11 | Runaway train, QNS&L Railway, Freight train LIM-55, Mile 67.20, Wacouna Subdivision | Dorée, Quebec | Loss of control |
| R09D0053 | 2009-09-09 | Non-main-track collision, VIA Rail Canada Inc., Locomotive 6425, VIA Rail Canada Inc., Montréal Maintenance Centre | Montréal, Quebec | Switching without air |
| R09T0057 | 2009-02-11 | Runaway and non-main-track train derailment, Southern Ontario Railway, 0900 Hagersville Switcher, Mile 0.10 and Mile 1.9 of the Hydro Spur | Nanticoke, Ontario | Securement |
| R08V0270 | 2008-12-29 | Non-main-track train runaway and collision, Kettle Falls International Railway, Waneta Turn Assignment, Mile 141.20, Kettle Falls Subdivision | Waneta, British Columbia |
Loss of control |
| R07H0015 | 2007-07-04 | Runaway rolling stock, CP, Runaway cut of cars, Mile 119.5, Winchester Subdivision | Smiths Falls, Ontario | Securement |
| R07V0109 | 2007-04-23 | Non-main-track train derailment, Kootenay Valley Railway, 0700 Trail yard assignment, Mile 19.0, Rossland Subdivision | Trail, British Columbia |
Loss of control |
| R06V0183 | 2006-09-03 | Runaway and derailment, White Pass and Yukon Railway, Work train 114, Mile 36.5, Canadian Subdivision | Log Cabin, British Columbia |
Loss of control |
| R06V0136 | 2006-06-29 | Runaway and derailment, CN, Freight train L-567-51-29, Mile 184.8, Lillooet Subdivision | Lillooet, British Columbia |
Loss of control |
| R05H0011 | 2005-05-02 | Runaway and main-track train collision, Ottawa Central Railway, Freight train 441, Mile 34.69, Alexandria Subdivision | Maxville, Ontario | Securement |
| R04V0100 | 2004-07-08 | Uncontrolled movement of railway rolling stock, CN, Train M-359-51-07, Mile 57.7, Fraser Subdivision | Bend, British Columbia |
Loss of control |
| R03T0026 | 2003-01-21 | Yard collision, CP, Car HOKX 111044, Mile 197.0, Belleville Subdivision, Toronto Yard | Agincourt, Ontario | Switching without air |
| R03T0047 | 2003-01-22 | Yard collision, CN, Tank Car PROX 77811, Mile 25.0, York Subdivision | Toronto, Ontario | Switching without air |
| R99D0159 | 1999-08-27 | Runaway cars, CN, Mile 69.4, Kingston Subdivision, Wesco Spur | Cornwall, Ontario | Securement |
| R98M0029 | 1998-09-24 | Main-track runaway, collision, and derailment, Matapédia Railway, CN train A402-21-24, Mile 105.4, Mont-Joli Subdivision | Mont-Joli, Quebec | Securement |
| R98M0020 | 1998-07-31 | Main-track runaway and collision, VIA Rail Canada Inc. passenger train 14 and an uncontrolled five-pak movement, Mile 105.7, Matapédia Railway, Mont-Joli Subdivision | Mont-Joli, Quebec | Securement |
| R97C0147 | 1997-12-02 | Runaway and derailment, CP, Train 353-946, Laggan Subdivision | Field, British Columbia |
Loss of control |
| R96C0172 | 1996-08-12 | Main-track collision, CN, Train 117 and an uncontrolled movement of 20 cars, Mile 122.9, Edson Subdivision | Near Edson, Alberta | Securement |
| R96C0209 | 1996-10-09 | Runaway cars, CP, CP 0700 yard assignment, Mile 166.2, Willingdon Subdivision, Clover Bar exchange track | Edmonton, Alberta | Securement |
| R96T0137 | 1996-04-24 | Runaway of 5 tank cars, CN, Mile 0.0, Hagersville Subdivision | Nanticoke, Ontario | Securement |
| R96C0086 | 1996-04-13 | Runaway train, CP, Freight train 607-042, Mile 133.0, Laggan Subdivision | Field, British Columbia |
Loss of control |
| R95M0072 | 1995-12-14 | Runaway cars, CN, Train 130-13, Mile 0.0, Pelletier Subdivision | Edmundston, New Brunswick |
Securement |
| R94V0006 | 1994-01-18 | Runaway train, CN, Freight train 459-GP-18, Mile 175, Grande Cache Subdivision | Latornell, Alberta | Loss of control |