Main-track derailment
Canadian National
Train M31451-28
Mile 144.19, Bala Subdivision
Falding, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At approximately 1050, Eastern Daylight Time, on 01 October 2010, Canadian National freight train M31451-28, proceeding southward from Capreol, Ontario, to Toronto, Ontario, derailed 21 cars just south of the James Bay Junction Road crossing at Mile 144.19 of the Bala Subdivision near Falding, Ontario. The derailed cars included 8 loaded tank cars containing non-odorized LPG (Special Dangerous, UN 1075) and 7 loaded tank cars containing fuel oil. A number of homes in the vicinity of the derailment were evacuated. There were no injuries and no product was released.
Ce rapport est également disponible en français.
Factual information
Canadian National (CN) train service design plans specify a horsepower to tonnage ratio (HPT) and identify scheduled lifts, set-outs and inspection points en route for a given train. CN train journals are checked against the designed HPT requirements to ensure that the train has adequate power to adhere to a predetermined schedule. CN freight train M31451-28 (the train) was a mixed conventional train (equipped with head-end power) which originated in Edmonton, Alberta and was destined for Toronto, Ontario. Between Winnipeg and Toronto, the train was to operate with a design HPT of 1.3. To maintain the ratio, operating crews may periodically place a locomotive off-line, or bring an additional locomotive online and ensure that the locomotives are properly setup to operate on a specific territory.
An outbound crew (crew 1) took control of the train at Hornepayne, Ontario and departed at 1750Footnote 1 on 30 September 2010. The train's locomotive consist comprised 4 head-end locomotives, each equipped with extended range dynamic brake (DB).Footnote 2 The consist was capable of generating up to 17,500 horsepower (hp) through 24 driving axles, but one of the locomotives was not online so the train's HPT was below the 1.3 minimum ratio. Consequently, the Rail Traffic Control (RTC) instructed crew 1 to bring the fourth locomotive online. Crew 1 responded that they were able to maintain track speed without the additional power and the train continued to Capreol, Ontario, without changing the locomotive setup.
Upon arriving at Capreol, crew 1 completed local switching then were relieved by the next crew (crew 2). During the crew change, crew 1 noted that the train was difficult to handle due to excessive slack action. Crew 2 took control of the train and were instructed by the RTC to bring the 4th locomotive online. Crew 2 complied and, during setup, left the DB online on all locomotives. With all 4 locomotives online, the locomotive consist was capable of producing up to 300,000 pounds of DB braking effort. The train departed Capreol en route to Toronto at 0717 on 01 October 2010.
The accident
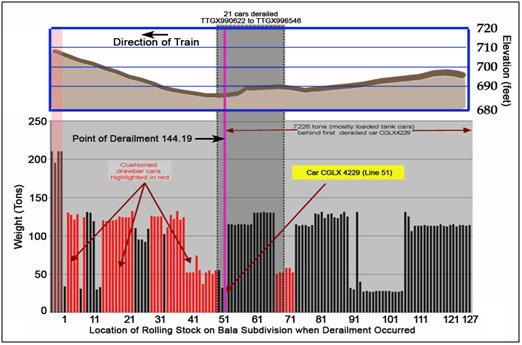
The train was hauling 127 cars (89 loads and 38 empties), weighed 12,909 tons and was 8,892 feet long. Thirty-nine of the first 49 cars were equipped with long travel hydraulic end of car cushioning devices (EOCCD); this included a block of 93 foot long empty multi-level auto carriers in the 39th to 49th positions from the head-end. The 50th and 51st cars were empty covered hopper cars. About 7200 tons of rolling stock trailed behind the 51st car. A block of twelve, short, empty aluminum covered hopper cars were located within the tail end portion of the train in the 95th to 106th positions.
Both members of crew 2 were familiar with the territory and qualified as both conductors and locomotive engineers. They were assigned to the Spare Board. In this case one was called and assigned as the train locomotive engineer. The conductor was well rested and fit for duty.
At approximately 1045 the train was proceeding southward at 35 mph on the Bala Subdivision towards Falding, Ontario (see Figure 1). The conductor briefly left the cab seating area and was not in a position to observe signals. At 1047:25, the train passed the southbound advance signal to Falding at Mile 144.6 with the train brakes released and the throttle in position 5. Shortly thereafter, the conductor returned to the cab seating area. Later, while passing Mile 144.0, the engineer could not recall the previous signal aspect and the crew prepared to stop the train in advance of the next signal location (Mile 142.8) as required by Canadian Railway Operating Rules (CROR). The locomotive engineer consulted his CN Best Practices Train Handling Guide for the Bala SubdivisionFootnote 3 which noted that for southbound trains, throttle manipulation is the preferred method of train control in the area, with no other restrictions.

The train began to slow as it entered an ascending grade. The engineer throttled off, then began to use dynamic brake (DB) and track grade to slow the train, but the train did not slow as expected. At 1049:09, the train was still travelling at 33 mph with 3⁄4-mile to the signal at Mile 142.8. The DB lever was moved from position 3 to 6 in two seconds and train speed dropped from 33 mph to 29 mph over the next 11 seconds.
At 1049:22, the crew felt a run-in of train slack and observed a 3 mph increase in train speed. The engineer reduced the DB, then varied it between positions 2 and 6 over the next 20 seconds. At 1049:42, a train-initiated undesired emergency brake application (UDE) occurred with the lead locomotive at Mile 143.25. The locomotive independent brake was bailed off and at 1050:02 the head-end came to rest at Mile 143.17, about 2000 feet north of the signal at Mile 142.8.
The crew completed the required emergency broadcasts and determined that 21 cars (lines 49 to 69) had derailed south of the James Bay Junction Road crossing at Mile 144.19. The derailed cars included 8 loaded LPG tank cars (special dangerous, UN 1075) and 7 loaded non-regulated fuel oil tank cars. Homes and businesses within a 1.6 km radius were evacuated until the site was secured. Environmental containment was established downstream of the accident site. There were no injuries and no product was released. Several loaded tank cars were damaged. The product was transhipped over the next few days. Most people were allowed to return home two days later.
The examination
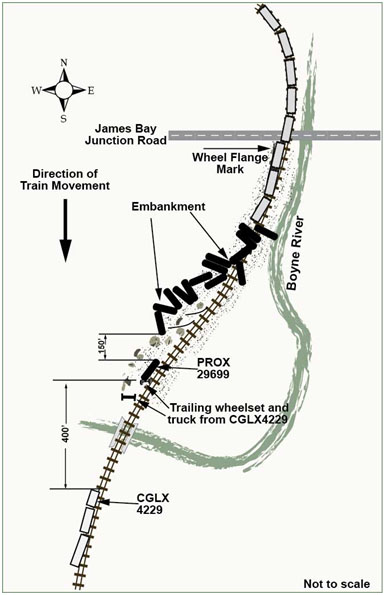
The derailed cars came to rest at the bottom of a sagFootnote 4 in curving, undulating territory.Footnote 5 Eleven feet south of the James Bay Junction Road crossing, in an exit spiral of a 5° right-hand curve (in the direction of travel) where there were flange marks on the head of the west rail (5 ties long). The marks dropped off the field side of the rail where the first wheel flange marks were observed on the ties between the rails and just beyond the tie plate ends on the field side of the west rail. The flange marks continued south into an area of destroyed track. No wheel flange marks were observed on the east rail head. About 105 feet south of the crossing, the west rail had rolled to the field side and the east rail was canted to the field side. Approximately 1 500 feet of track was destroyed.
The derailed cars included TTGX 99062 - an empty multi-level auto carrier (line 49), NAHX 551057 - an empty 65 foot 32 ton covered hopper car (line 50), CGLX 4229 – an empty 40 foot long 27 ton aluminum covered hopper car (line 51), 15 loaded tank cars (lines 52 to 66), and 3 empty multi-level auto carriers (lines 67 to 69).
The 49th to 51st cars had derailed upright and remained coupled to the head-end portion of the train. The trailing truck of TTGX 99062 had derailed as the west side wheels dropped into gauge between the rails and the east wheel remained on the rail head. The lead truck of NAHX 551057 derailed with the east side wheels dropping into gauge and the west side wheels remaining on the rail head. The trailing truck of NAHX 551057 and lead truck of CGLX 4229 both dropped into gauge and spread the rail. The trailing truck of CGLX 4229 had displaced from under the car and came to rest just north of a short trestle bridge; its trailing wheel set was located 400 feet north, under the lead end of the following car PROX 29699 (line 52). The top portion of the knuckle on the lead end of PROX 29699 had broken; the fracture surface exhibited brittle overstress characteristics; no casting defects were observed.
The following 15 loaded tank cars (52nd to 66th) had rolled and jackknifed in various orientations predominantly to the west of a 350 foot portion of elevated tangent track. In this area, the west rail had rolled and shifted to the west. The derailed tank cars slid down an embankment and came to rest in a swampy area where the track entered a 2° left-hand curve. The 66th car came to rest upright on the bank of the Boyne River east of the tracks. The 67th to 69th cars had derailed upright on the web of the canted west rail, and on the ties between the rails (see Figure 2).
Track information
The Bala Subdivision is Class 4 single main track, which extends from Toronto (Mile 0.0) northward to Capreol (Mile 276.1). In the vicinity of the derailment, between Mile 142.3 and Mile 160.3, zone speed for freight trains had been permanently reduced to 40 mph (Class 3 track standards). Movements on the Bala Subdivision are governed by the Centralized Traffic Control System (CTC), as authorized by the Canadian Rail Operating Rules (CROR) and supervised by a rail traffic controller (RTC) in Toronto.
Between Boyne (Mile 146.1) and James Bay Junction Road (Mile 144.19), a generally descending track gradient fluctuates between 0.0 and -0.6 % through a series of 5 curves. James Bay Junction Road crosses the track in the exit spiral of a 5° right-hand curve. From the crossing to the north siding signal at Falding (Mile 142.8), the track ascends a roughly 0.8 % grade.
In the vicinity of the derailment, the track was visually inspected in accordance with Transport Canada (TC) approved Rules Respecting Track Safety (Track Safety Rules). The most recent visual inspection occurred just prior to the accident on 01 October 2010 with no defects observed. A rail flaw detection test was last conducted on 01 September 2010, with no exceptions noted, and the most recent track geometry inspection was conducted on 19 September 2010.
The track geometry car recorded two defects in the vicinity of the derailment between Mile 144.1689 and Mile 144.1625: an urgent Warp 31 spiral defectFootnote 6 of 1 1⁄2 inches over 3 feet, and a near-urgentFootnote 7 WRP62SPR (Warp 62 spiral)Footnote 8 defect of 1 7⁄8 inches over 15 feet. A 25 mph temporary slow order for freight trains was applied and repairs were completed on the same day. Local surfacing was done on 21 September 2010 and the speed restriction was removed.
In-train forces
Newer locomotives, such as the occurrence locomotives, are equipped with extended range DB and are capable of producing significant braking forces. For conventional trains, these DB braking forces are focused at the head end which generally results in the train bunching tightly together as train slack compresses. In general, when train automatic air brakes are used, the air brakes apply throughout the train which normally keeps the train stretched. DB was used exclusively by the locomotive engineer in his attempt to stop the train before passing the signal.
Train operations have changed significantly in recent years. Before the mid-1990s, an average train in main-track service was about 5000 feet long and weighed 6000 to 7000 tons. Today 12 000 foot / 12 000 ton trains are not unusual. The significant increase in average train length and weight has been associated with increases in normal in-train forces for conventional trains equipped with head-end power. When the head-end power has extended range DB, in some situations, the use of DB can further increase in-train forces. Under these conditions, car placement or marshalling plays an important role in minimizing the in-train forces.
In 1992, the Association of American Railroads (AAR) made available a train manual to provide a basic understanding of the parameters that affect train safety due to train make-up.
AAR R-802 Train Make-Up ManualFootnote 9 discusses excessive train forces. It identifies changes in gradient as an important transient force that can be further magnified in the presence of horizontal curves. The manual states that tonnage should not be concentrated on the rear of a train in undulating terrain. Power and braking adjustments must be small and gradual.
A train moves as a locomotive develops tractive effort. It is slowed by DB, air braking and rolling resistance of the rolling stock. When a train is operating on tangent track with the slack stretched (draft), the drawbar forces act along the centreline of the track. When a car negotiates a curve, lateral forces are transmitted at the wheel-rail interface as the curved rail alters the wheel tendency to roll straight ahead. This occurs primarily through the wheel flange contacting the gauge face of the high rail. When the train slack is bunched (buff), buff forces tend to push the train outward. If wheel unloading occurs during this time, a wheel lift derailment can occur.
Lateral and vertical wheel forces always exist when a vehicle is moving. The lateral to vertical ratio (L/V) is the lateral force pushing outward against the rail divided by the vertical force pushing downward on the top of the rail. The tendency for the wheel to lift or climb the rail increases as the L/V ratio increases. The L/V ratio will increase if the lateral force increases and the vertical force remain constant, or if the vertical force decreases and the lateral force remain constant. A wheel L/V ratio of >0.82 is known to be sufficient to cause wheel lift while an L/V ratio of >0.75 is known to be sufficient for a wheel to climb a worn rail.Footnote 10
The AAR R-802 Train Make-Up Manual also considers special car cases such as EOCCD equipped cars and cars with extremely low tare weights. EOCCDs add to train slack and can greatly increase in-train forces. Specifically, the manual states that large blocks of EOCCD–equipped cars should not be placed ahead of large blocks of loaded cars with conventional draft gears.
It also notes that cars with extremely low tare weights can be problematic when placed ahead of heavier cars. Specifically, short light cars are known to be susceptible to string-lining and jack-knifing when placed ahead of significant trailing tonnage. When empty, the low vertical forces acting on such cars magnify L/V ratios when coupler jack-knifing is induced by high longitudinal buff forces. Under these circumstances, these cars are susceptible to wheel climb type derailments on curves when coupled ahead of significant trailing tonnage. The position of the occurrence consist in relation to trailing tonnage and track gradient is presented in Figure 3.
CN train marshalling
CN freight trains are made up using destination block marshalling where blocks of cars are placed in the train in a manner that expedites their set-out or pick-up along the train's route.
CN uses a computerized system that identifies any train marshalling that does not comply with either the Transportation of Dangerous Goods Regulations or CN's General Operating Instructions (GOIs). CN's GOIs have placement restrictions (for example, dimensional loads) and trailing tonnage restrictions for certain types of cars (for example, skeleton cars, spine cars). However, at the time of the accident, there were few operational restrictions on the marshalling of most types of freight cars, whether empty or loaded.
Due to a number of TSB investigations that involved longer, heavier trains and the inappropriate management of in-train forces, the Board included this safety issue on its Watchlist (March 2010). The Watchlist states that “inappropriate handling and marshalling can compromise the safe operation of longer, heavier trains” and calls on railways to “take further steps to ensure the appropriate handling and marshalling of longer, heavier trains.”
In July 2010 CN began developing train marshalling rules primarily for conventional trains equipped with head-end power. The rules are based on industry practice and accident history and focussed primarily on train weight distribution in an effort to minimize in-train forces. CN proposed the following train marshalling rules:
- Rule 1, Tail End Heavy: 33% or more of the train weight in the rear 25% of the train
- Rule 2, Empty Block Stability: Solid block of >10 light cars
- Rule 3, Solid block of >20 loads trailing a solid block of >20 light cars
- Rule 4, Excessive EOCCD cars; >120/train
- Rule 5, Excessive EOCCD cars on head-end. Trains with >80% of non CC's in rear 25%
- Rule 6, Long Car-Short Car, Long Car >= 79 feet coupled to a short car <47 feet
Additional rules subject to train tonnage criteria will be customized to the territory.
CN began with partial implementation. It initially tested then, in December 2010, and implemented Rules 1, 2 and 4 on the Kingston and Wainwright Subdivisions with the goal of eventually implementing the marshalling rules system wide. In addition, CN restricted maximum train length to 8500 feet for conventional trains on both subdivisions and began to introduce the use of distributed power. While the occurrence train exceeded length criteria, the CN marshalling rules were not in effect on the Bala Subdivision at the time of the accident. Furthermore, there is no rule governing placement of a short, light freight car.
However, some positive steps have been taken by different stakeholders to address the issues of proximity.
Other train marshalling
Canadian Pacific Railway (CPR) considers weight distribution during train marshalling. CPR has developed and implemented Train Area Marshalling (TrAM), a proprietary computer–based train marshalling system, to minimize the effect of in-train forces. TrAM rules include trailing tonnage limits for specific types of car equipment. The limits vary depending on factors such as type of car, length of the car, weight of the car (content plus tare weight), length of adjacent car, as well as curvature and grade of the track over which the car will operate.
The system also considers and assists with the placement of cars with EOCCDs and DP consists. TrAM requires that freight trains be made up, to the maximum extent practicable, with the loads located closest to the locomotives. For mixed conventional trains, the marshalling of heavy blocks of cars at the rear of the train is prohibited unless blocks ahead are equally as heavy. Light cars (empties) or blocks of light cars are marshalled as close as possible to the rear unless the cars behind are also relatively light. While CPR uses destination block marshalling, it does not take precedence over TrAM marshalling restrictions.
Train dynamics simulation
A train dynamics simulation was conducted to evaluate the use of DB, the magnitude of longitudinal draft forces generated and any associated transformed L/V ratios acting on the occurrence train under the accident conditions. To expedite the analysis, the simplified model did not include the additional effect of slack run-in from the EOCCD located at the head-end of the train. Consequently, the longitudinal force values derived are considered to be conservative.
The simulation determined that:
- The 51st car CGLX 4229, a short, light, empty car, was likely the first car to derail. The highest longitudinal forces were recorded nearest the head-end of the train with more moderate forces acting on the first derailed car.
- Comparison of the in-train forces and transformed L/V ratios at car CGLX 4229 (51st) and PROX 29699 (52nd) demonstrate the importance of car weight. The in-train forces were very close at the adjacent cars, but the transformed L/V ratios were very different. The transformed L/V ratio recorded at the very light empty car (51st) was 1.08, which exceeded wheel climb criteria, while the L/V ratio for the heavily loaded tank car (52nd) was 0.31 which was within safety limits.
- The undulating track grades affected the in-train force distribution.
- For the occurrence train with 4 locomotives and 24 DB operative axles located at the head-end, a moderate run-in force of 129 kips produced a wheel L/V ratio of 1.08 at car CGLX 4229. Under a car body jack knife condition, the forces acting on a car are amplified, leading to situations where a moderate run-in force can produce an elevated L/V. When the forces act on a short light car, a wheel can be induced to climb the rail or to roll the rail over.
- For the occurrence train with 3 locomotives and 18 DB operative axles located at the head-end, a moderate run-in force of 105 kips produced a wheel L/V ratio of 0.88 at car CGLX 4229. This L/V ratio is still at a level that is considered to be at risk for a wheel climb derailment.Footnote 11
- When 2 of the locomotives were placed midway in the train (distributed power), a buff force of 40 kips produced a wheel L/V of 0.41 at car CGLX 4229.
- While measured DB peaks were only moderately elevated, the non-standard use and application of DB was a contributing factor in this derailment.
CN Locomotive Engineer Operating Manual
The CN Locomotive Engineer Operating Manual (August 2010Footnote 12), Section G Train Handling in part, provides the following instructions with regards to the use of DB:
- Section G1.2 standardizes the best practices for train handling throughout CN.
- Use forward planning for planned stops and speed control;
- Make only incremental/gradual throttle and brake adjustments;
- Control speed using throttle manipulation to the greatest extent possible;
- Select and adjust the throttle, dynamic brake, and air brake in a manner which minimizes in-train and track-train forces; and
- Allow slack to gradually adjust within the train before increasing throttle, dynamic brake, or air brake applications.
- Section G2.12 states that dynamic braking is an excellent method of speed control, but it is capable of generating high in-train and track-train forces. Because DB concentrates the retarding force at the head-end of the train, there are limits to the amount of braking which should be applied using DB. To avoid excessive force, it may be necessary to use a combination of DB and automatic brake, and/or to implement speed control tactics further in advance. For any given DB handle position, maximum retarding forces occur in the 5 to 30 mph speed range. Extra care must be exercised in this speed range. Adjustments of the DB handle are to be made in a smooth and steady manner.
The key process steps in applying dynamic brake are as follows:- When changing from power to DB, reduce the throttle to IDLE one position at a time, pausing briefly in each throttle position. Once the throttle is in IDLE, wait 10 seconds, then move the DB handle to SET-UP position. The pause allows current in the traction motor fields to dissipate, prevents a surge of retarding force, and allows the train slack to adjust.
- To initiate dynamic braking, advance the DB handle past SET-UP in small, incremental moves, allowing the slack to bunch against the locomotive consist.
- Once the slack is bunched against the locomotive consist, make further adjustments of the DB handle in a smooth and steady manner, allowing at least 30 seconds in progressing to maximum braking effort.
- If the wheel slip or brake warning light illuminates, reduce the dynamic braking effort until the light extinguishes. If the light remains illuminated, stop the train and inspect the locomotive consist.
- To prevent slack from running out when coming to a final stop, gradually apply the independent brake. The DB handle may be moved to the OFF position once the independent brake becomes effective. The train brakes may also need to be applied to prevent the slack from running out when stopping on an ascending grade.
- Section G2.13 identifies that locomotives can develop very high levels of DB retarding forces capable of damaging the track structure and/or generating excessive buff forces in the train. Either situation can lead to a derailment. The use of DB must be limited. To respect these limitations, the locomotive engineer must employ speed control strategies farther in advance, and/or use a combination of DB and automatic brake.
- Section G2.13 (1) restricts a head-end locomotive consist to 18 axles with operative DB. When operating one or more alternating current (AC) locomotives, the maximum number of operative DB axles in the consist must not exceed 12.
- Section G3.3 discusses jackknifing. Operators are instructed to exercise extreme caution when making bunched stops or decreasing speed giving due consideration to grade, curvature and weight distribution. Operators are instructed to exercise care when using DB without train air brakes to effect a slow down or stop, particularly with 4 or more locomotives in the consist.
CN locomotive engineer instruction on train nandling
Locomotive engineers are instructed and tested on train handling rules as part of locomotive engineer training. Hands-on training typically occurs in the region where the locomotive engineer works. During hands on training, locomotive engineer trainees obtain experience in train setup and handling. Crews are provided with CN Best Practices Train Handling Guide for the respective subdivision to become familiar with controlling the train in the most efficient manner. To conserve fuel and reduce wear on brake components, crews are taught to plan ahead and to use throttle manipulation and DB as the preferred methods of train control.
Crew 2 had received instruction on the use of dynamic brake and on the restriction for the total number of axles at the head-end with operative DB. The locomotive engineer had operated trains south of Parry Sound on 18 previous occasions, several of which were M314- series or similar mixed merchandise trains. The conductor had not yet been assigned to operate a train as a qualified locomotive engineer. Conventional CN trains in the Great Lakes Region rarely require more than 2 or 3 locomotives to meet HPT requirements. Consequently, crews seldom operate a train which exceeds 18 head-end axles in total. Prior to this accident, crew 2 had never operated a train that required them to apply the 18 axle DB restriction.
Spare board employees
Spare board conductors are not assigned to specific trains but are called to fill vacancies, subject to industry work-rest rules. Crews are called for assignments on the basis of seniority in a “first in-first out” basis. Employees who are lower on the spare board are generally less able to predict their next work assignment compared to those at the top of the list. Spare board employees can, to some degree, anticipate when they are likely to be called to work. Spare board conductors who are also qualified as locomotive engineers can be called at any time to operate an assignment in an engineer capacity; however, these employees will not be called to operate trains in the same frequency as employees in the engineer pool.
Work/rest rules and sleep-wake schedule for locomotive engineer
In accordance with the Transport Canada's (TC) Work/Rest Rules for Railway Operating Employees (Work/Rest Rules), running trades employees receive fatigue management training and are responsible for ensuring they are ready and rested when called to work. If an employee is listed as available to work a shift and then refuses a shift, the employee can face some form of company intervention.
In November 2007, the Railway Safety Act Review Panel made the following recommendation:
(43) Fatigue management is dealt with in complimentary ways, such as work/rest rules, fatigue managements plans, and terms and conditions of employment.
- The current work /rest rules do not provide a satisfactory baseline framework for managing risks associated with fatigue in rail operations. The rules should be amended to better reflect current science on fatigue management.
- A robust system of fatigue management plan is needed. Transport Canada should audit them as it does safety management system plans.
- Fatigue management is also an issue that railways and employees should address in the establishment of terms and conditions of employment.
The Fatigue Management Plan Requirements and Assessment GuidelinesFootnote 13 were approved in September 2010. The guidelines provide detailed recommendations for the development and assessment of fatigue management plans and procedures.
The locomotive engineer was off duty for over 36 hours prior to the occurrence trip. Between night sleep and afternoon napping, the locomotive engineer normally obtained about 7.5 hours of sleep each day. On the night before the occurrence, the locomotive engineer went to bed shortly after 0100 and was awakened by a child crying at approximately 0300. He obtained between 1 and 1 1⁄2 hours of sleep during this sleep period. He remained awake and received his call for work at 0445 hrs. He began his shift at 0625.
Sleep duration, fatigue and performance
Most people require 7.5 to 8.5 hours of sleep for each 24 hour period.Footnote 14 Research has reliably demonstrated that shortening a person's total sleep time to less than one's biological need results in fatigue and performance decrements.Footnote 15, Footnote 16, Footnote 17 Fatigue will impair many facets of human performance, including reductions in cognitive, attention and memory performance.Footnote 18, Footnote 19, Footnote 20 A 1997 review of 100 railway accidents and near accidents determined that a lack of alertness was the most important single contributor.Footnote 21 Train operator studies have shown that fatigued train operators are less efficient. Specifically, the studies determined that:
- Fuel consumption is higher, heavy brake applications are more frequent, and dynamic brake and throttle manipulation are reduced. The heavy brake applications typically occur when train operators are trying to make sudden, safety-critical speed reductions as a result of failure to adequately plan for upcoming track features requiring the train to slow down. In general terms this means that fatigue affects the ability to plan ahead and influences operator braking behaviour.Footnote 22
The frequency and magnitude of speeding by railway engineers increases with fatigue. This is likely due to fatigue leading to a reduction in planning (i.e. a failure to anticipate and prepare for upcoming track features) and would lead to either a speeding or braking error (e.g. heavy brake application).Footnote 23
Other related accidents
On 27 October 2007, CN train A41751-26 (train 417), operating westward on the Edson Subdivision passed a stop signal and collided with eastbound CN train M34251-26 that was entering a siding at Peers, Alberta. Twenty-seven cars and 2 locomotives derailed without serious injury or release of dangerous goods (TSB report No. R07E0129). The investigation determined one of the factors contributing to the derailment was that “the crew of train 417 was insufficiently rested to be engaged in safety critical tasks.”
Since 2000, the TSB has conducted 11 derailment investigations that involved high in-train forces in long CN trains (see Appendix A). In each case, the Board determined that train marshalling and the management of in-train forces were contributing factors. While most trains were marshalled in accordance with railway and regulatory requirements in place at the time, they were not configured in a way that effectively managed in-train forces.
Analysis
There were no track or rolling stock defects that were considered causal to the accident. The fractured knuckle on the lead end of PROX 29699 failed as a result of the derailment and was not considered causal. The analysis will focus on crew actions, train marshalling, dynamic brake setup in high curvature undulating territory and in-train forces.
The accident
The wheel flange marks observed at the bottom of a sag in the exit spiral of a 5° curve were indicative of a wheel climb initiated derailment which can occur when a wheel L/V force exceeds derailment criteria. The train separation occurred between the 51st and 52nd car and the trailing truck of the 51st car (CGLX 4229) had displaced from under the car and was located 400 feet north under the 52nd car. This suggests that a wheel set in the trailing truck of CGLX 4229 was likely the first to derail. Once CGLX 4229 had derailed, the track sustaineddamage and the train eventually separated which caused the emergency brake application. Consequently, a total 21 cars derailed and came to rest in various positions.
The highest longitudinal forces were recorded nearest the head-end of the train with more moderate forces acting on the first derailed car. This suggests that both the placement of CGLX 4229 (a single empty, light, 40 foot long car) in the 51st position ahead of 7200 trailing tons and the undulating track played a role. Train dynamic simulation confirmed that CGLX 4229 was likely the first car to derail when a moderate run-in buff force of 129 kips produced a wheel L/V of 1.08 at the trailing truck, a value which exceeds derailment criteria. The undulating track grades also affected the in-train force distribution and, when combined with the non-standard use of DB, exacerbated the buff force at the derailment location. The train derailed, while stopping using DB, when a moderate run-in buff force of 129 kips produced a wheel L/V of 1.08 at the trailing truck of car CGLX 4229, a very short, light, empty car marshalled ahead of 7200 tons, as it exited a 5° curve in a sag.
The in-train buff force that initiated the derailment was preceded by an unplanned dynamic braking event. The train approached Falding at about 1045 and the conductor briefly left the cab seating area and was not in a position to observe signals. At 1047:25 the train passed the southbound advance signal at Mile 144.6 with the train brakes released and the throttle in position 5, after which the conductor returned to the seating area. Because the locomotive engineer could not recall the previous signal and the conductor was not present when the train had passed it, crew 2 could not positively identify the signal and prepared to make an unplanned stop, in advance of the next signal, using DB. However, the locomotive engineer applied the DB in a rapid non-standard fashion and did not account for a run-in of train slack from the trailing tonnage which was still on a descending grade, both of which increased the in-train forces.
Operator fatigue
The missed signal indication and non-standard manner in the application of DB were consistent with errors that commonly occur due to fatigue. A review of the locomotive engineer's sleep history confirmed he had less than 2 hours of sleep in the preceding 24 hours. This is far less than the required 7.5 to 8.5 hours which indicates that the locomotive engineer was likely in a fatigued state, a condition that is known to compromise cognitive, attention and memory performance. The locomotive engineer recognized he was tired when accepting the assignment, but knew that refusing an assignment when called could result in loss of wages due to a missed trip and/or potential company discipline. Furthermore, because he was a spare board locomotive engineer, he had reduced opportunities to operate trains that were marshalled like the occurrence train and was operating a train with known train handling challenges south of Parry Sound for the first time. The locomotive engineer was insufficiently rested to be engaged in safety critical tasks. His fatigued state was compounded by the challenge of operating an unfamiliar train during an unplanned braking event in undulating territory with a number of curves.
Modern family life does not always integrate well with the work schedule of a conductor or locomotive engineer. Many families now have more than one income-earning parent, with home and childcare duties shared more equitably. In this environment and even with the best of intentions, it is inevitable that on occasion an employee with family demands may not be fully rested when called to work. This especially applies to train crews that are assigned to the spare board because the work assignments are not as easy to predict in order to plan rest. If an employee turns down a trip, they lose the trip and are returned to the bottom of the spare board which results in a loss of wage. Crews are expected to be rested and ready for work whenever they are called, subject to Transport Canada work-rest regulations. Companies expect that when called for work, typically with 2 hour notice, operating employees accept the work, arrive on time and be fit to perform their duties safely for up to 12 hours. If the employees do not accept the work, they are likely to face some form of company discipline. Although the industry was in the process of implementing new fatigue management guidelines, at the time of this occurrence it was still left to employees to determine whether they were fit to work. When faced with loss of wage and/or potential company discipline, there is an increased risk that a fatigued employee will accept work, compromising safe train operation.
Train marshalling
Train marshalling, weight and length each affect the magnitude of in-train forces. For conventional mixed commodity trains, industry train make-up guidelines published in 1992 identified that placement of cars equipped with EOCCD at the head-end of a train with heavy trailing tonnage as likely to generate elevated in-train forces. Such forces are increased when locomotives generating high DB forces are marshalled at the head-end and braking effort is not controlled by limiting the number of operative DB axles. The guidelines also note that the placement of very light cars ahead of significant trailing tonnage is problematic and identifies undulating and high curvature territory as troublesome. All of these factors were present in this occurrence.
The TSB train dynamic simulation did not include the magnifying effects of the EOCCD cars with regards to in-train forces. However, even though the assumed values are conservative, wheel climb derailment conditions were still achieved. While the train was marshalled in accordance with CN's GOIs, it was not marshalled in a manner that considered track profile or the placement of CGLX 4229 (a short, light, empty car) in order to minimize in-train forces.
Over the last 10 years, the Board has investigated 11 other CN derailments where train marshalling and the management of in-train forces were contributing factors. Subsequently, inappropriate train handling and marshalling has been flagged on the TSB's Watchlist as one of 9 safety issues posing the greatest risk to Canadians.
CN began developing train marshalling rules primarily for conventional trains equipped with head-end power in July 2010 and also began to increase the use of distributed power. CN initially tested Rules 1, 2 and 4 and restricted maximum conventional train length to 8500 feet on the Kingston and Wainwright Subdivisions before fully implementing these rules on both subdivisions in December 2010. While the occurrence train exceeded length criteria, the rules were not in place at the time of the accident and did not apply to the Bala Subdivision. Even if the rules were in effect, CN has no rule governing placement of a single short, light, empty, freight car such as CGLX 4229.
There were alternatives for marshalling CGLX 4229 that could have minimized in-train forces. The car could have been marshalled with a similar block of cars located near the rear of the train which would have made the train less vulnerable to in-train forces. Alternately, the train could have been set up using distributed power. Dynamic simulation determined that when the train was set up with 2 head-end locomotives and 2 mid-train locomotives, the run-in buff force was reduced to 40 kips and resulted in a wheel L/V of 0.41 at the trailing truck of car CGLX 4229, values that were well below derailment criteria. In the absence of marshalling rules that govern the placement of single short, light, empty freight cars in conventional trains with consideration for geography, train length, weight and trailing tonnage, there is an increased risk of derailment due to in-train forces.
Dynamic brake setup
At Capreol, crew 2 was instructed to bring the 4th locomotive online. Crew 2 complied and, during setup, left the DB on all locomotives. With all 4 locomotives online, the locomotive consist had 24 DB operative axles and was capable of producing up to 300,000 pounds of DB braking effort. While this brought the train in line with the designed HPT minimum requirements, it placed the train in conflict with the CN GOI restricting the number of DB operative axles to 18. However, neither the train crew nor the train operations personnel in Capreol were sufficiently familiar with CN GOI's to recall that the setup restricted the number of DB operative axles to 18. Because only a few trains operate through this territory with excess DB axles, these personnel receive little if any practical experience in the application of the relevant GOI.
When safety critical activities are infrequently performed, there is a risk that they may be forgotten. “Defense-in-depth” models are predicated on maintaining multiple lines of administrative and physical defences to prevent an error of omission. While CN train documents clearly alert crews to a number of operational restrictions, including the required HPT, there is no alert to remind crews to review DB restrictions when present. When crews are required to recall an operating restriction for a locomotive setup that they rarely encounter or use, there is an increased risk that the restriction will not be properly applied.
Because crew 2 did not comply with the CN GOI restricting the number of DB operative axles to 18, the train had 24 DB operative axles, which increased the DB capacity to 25% over the maximum. Dynamic simulation conservatively determined that for the occurrence train, a moderate run-in force of 129 kips produced a wheel L/V ratio of 1.08 at car CGLX 4229. However, when the simulation was run with 3 locomotives and 18 DB operative axles located at the head-end, a moderate run-in force of 105 kips produced a wheel L/V ratio of 0.88 at car CGLX 4229. This is still a level that is considered to be at risk for a wheel climb derailment. Therefore, although DB-setup instructions were not followed, had the maximum number of DB-operative axles been limited to 18 and all other variables remained consistent with the best case scenario, CGLX 4229 would have still experienced L/V forces at risk for a wheel climb derailment.
Findings
Findings as to causes and contributing factors
- The train derailed, while stopping using dynamic brake, when a moderate run-in buff force of 129 kips produced a wheel L/V of 1.08 at the trailing truck of car CGLX 4229 (a very short, light, empty car) marshalled ahead of 7200 tons, as it exited a 5° curve in a sag.
- Because the engineer could not recall the previous signal and the conductor was not present when the train had passed it, crew 2 could not positively identify the signal and prepared to make an unplanned stop, in advance of the next signal, using Dynamic Brake.
- The engineer applied the Dynamic Brake (DB) in a rapid non-standard fashion and did not account for a run-in of train slack from the trailing tonnage which was still on a descending grade, both of which increased the in-train forces.
- The locomotive engineer was insufficiently rested to be engaged in safety critical tasks. His fatigued state was compounded by the challenge of operating an unfamiliar train during an unplanned braking event in undulating territory with a number of curves.
- While the train was marshalled in accordance with Canadian National's General Operating Instructions (GOI), it was not marshalled in a manner that considered track profile or the placement of CGLX 4229 in order to minimize in-train forces.
Finding as to risk
- Given that it is left to employees to determine whether they are fit to work, when faced with loss of wage and/or potential company discipline, there is an increased risk that a fatigued employee will accept work, compromising safe train operation.
- In the absence of marshalling rules that govern the placement of single short, light, empty freight cars in conventional trains with consideration for geography, train length, weight and trailing tonnage, there is an increased risk of derailment due to in-train forces.
- When crews are required to recall an operating restriction for a locomotive setup that they rarely encounter or use, there is an increased risk that the restriction will not be properly applied.
Other finding
- Although DB-setup instructions were not followed, had the maximum number of DB operative axles been limited to 18 and all other variables remained consistent with the best case scenario, CGLX 4229 would have still experienced L/V forces at risk for a wheel climb derailment.
Safety action taken
Transport Canada
On 23 February 2011, the Minister of Transport approved revisions to the Work-Rest Rules for Railway Operating Employees. The railway companies were asked to file their revised fatigue management plans by November 2011.
In February 2011, TC began a Canada-wide study of long-train operations to develop policies for train marshalling and handling. This study will be completed in two years and will develop science-based data. The Phase I preliminary results and recommendations will be available in late 2011. In addition, TC initiated a multi-stakeholder research project that will examine in-train forces. The industry is moving forward on improved software, train marshalling and locomotive power distribution to better control the in-train forces that affect longer, heavier trains over various terrains. Based on the results of these studies and on industry movement on this issue, TC will determine the appropriate regulatory and/or safety action to be taken.
Canadian National
CN implemented a number of practices and programs to mitigate crew fatigue. CN's Fatigue Management Plan (FMP) lays out the initiatives related to education, medical monitoring, alertness strategies, work scheduling, rest facility standards and locomotive work environment. The FMP is currently being enhanced with additional features as part of the recent amendments to the Work/Rest Rules. In addition, CN and its operating unions embarked on a pilot project in a number of terminals to assess the scheduling for unassigned service.
CN implemented marshalling Rules 1, 2 and 4 across its entire Canadian core route.
CN placed additional emphasis on ensuring that train crews comply with rules, including those that are infrequently encountered. A major part of this initiative is CN's Efficiency Test Program. Over 900 tests are performed by supervisors each day to ensure compliance with safety practices, policies and operating rules. All test results are documented in CN's centralized Performance Monitoring and Rules Compliance (PMRC) system. The program was enhanced with the addition of a series of “dynamic” e-tests in which scenarios, including many that are not regularly encountered, are simulated to ensure proper and compliant responses.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
Appendix A – Other related TSB investigations
The TSB has conducted investigations into the following derailments:
- R10T0056 - On 30 March 2010, CN freight train M37631-30, proceeding eastward derailed 4 locomotives and 11 cars near the GO Train station at Mile 1.40 of the York Subdivision in Pickering, Ontario. The investigation determined that high in-train buff forces generated excessive lateral forces between the second and third isolated locomotives resulting in track panel shift, rail roll over and derailment. Locomotives with no coupler alignment control magnified the lateral drawbar force and produced a high lateral/vertical ratio that exceeded derailment criterion. The train was marshalled in accordance with CN and regulatory requirements.
- R09T0092 - On 21 March 2009, CN freight train M36231-20, proceeding eastward at about 50 mph, derailed 6 cars at Mile 247.20 of the Kingston Subdivision, near Brighton, Ontario. The train was powered by three head-end locomotives hauling 137 cars (75 loads and 62 empties). It was approximately 8850 feet long and weighed about 11 845 tons. A moderate run-out of train slack resulted in a broken knuckle on the 107th car. The train separated into a head-end portion of 107 cars and a tail-end portion of 30 heavily loaded cars. The heavier tail-end portion subsequently collided with the head-end and caused the derailment. The investigation determined that the train was operated in accordance with company and regulatory requirements, but it had not been configured in a way that effectively managed in-train forces.
- R07D0009 - On 12 February 2007, CN freight train M31031-10 derailed 8 cars near Drummondville, Quebec. A broken knuckle on the 75th car caused an emergency brake application to propagate to the head-end. The train consisted of 5 head-end locomotives and 105 cars (80 loads and 25 empties), was approximately 7006 feet long and weighed about 10 815 tons. The investigation determined that train marshalling was a contributing factor.
- R07T0110 – On 28 April 2007, CN freight train M36321-26 derailed a Herzog track maintenance machine and 21 empty multi-level cars at Cobourg, Ontario. The train consisted of 3 head-end locomotives and a mix of 84 empty and loaded cars. It was 9602 feet long and weighed about 9000 tons. The investigation determined the positioning of a car equipped with non-standard couplers and 45 empty EOCCD cars at the head-end of the train with significant trailing tonnage was a contributing factor.
- R07T0323 – On 30 October 2007, CN freight train M38461-29 derailed while stopping to set off a block of intermodal cars at Malport, Ontario. The train consisted of 4 head-end locomotives and 131 cars (59 loads and 72 empties). It was approximately 7839 feet long and weighed about 7810 tons. The investigation determined the placement of equipment with non-standard couplers at the head-end of a train with significant trailing tonnage, was a contributing factor.
- R05V0141 – On 05 August 2005, CN freight train A47151-05 derailed nine cars, including one load of sodium hydroxide (UN 1824) and 8 empty cars near Garibaldi, British Columbia. Approximately 40 000 litres of product spilled into the Cheakamus River, causing extensive environmental damage. The train consisted of 5 head-end locomotives, 144 cars (3 loads and 141 empties), and 2 remote locomotives behind the 101st car. It was about 9340 feet long and weighed approximately 5002 tons. The investigation determined that the combination of excessive locomotive tractive effort and trailing tonnage, along with long–short car coupling, produced high lateral forces and a correspondingly high lateral/vertical ratio and wheel lift, causing the train to string line the curve.
- R02C0050 – On 08 July 2002, CN freight train A44251-08 derailed 2 locomotives and the first 27 car bodies. Under braking, the non-alignment couplers on the derailed locomotives permitted maximum drawbar angles of approximately 19 degrees. Buff forces translated through these couplers generated lateral forces which were sufficient to cause rail roll and wheel lift, leading to the derailment.
- R02W0060 – On 26 April 2002, CN freight train E20131-24 was departing Winnipeg, Manitoba, along the north main track of the Redditt Subdivision. Eight cars derailed as the train traversed a crossover with the DB applied. The train consisted of 3 locomotives and 85 cars (76 loads and 9 empties), was 5412 feet long, and weighed 9363 tons. The investigation determined that the run-in of slack from significant trailing tonnage, combined with a sustained DB level, generated buff forces severe enough to initiate wheel lift and to derail an empty 80-foot bulkhead flat car.
- R01M0061 – On 06 October 2001, CN freight train M30631-05 derailed 15 cars after striking an automobile at a farm crossing in the township of Drummond New Brunswick. Seven of the derailed cars were tank cars carrying liquefied petroleum gas (UN 1075). The train consisted of 3 head-end locomotives, 130 cars (60 loads and 70 empties), was about 8700 feet long and weighed approximately 10 000 tons. The investigation determined that an undesired emergency brake application (UDE) occurred when the train struck the automobile. Due to the track profile and train configuration, there was excessive run-in which generated high buff forces, resulting in rail rollover and the derailment.
- R01T0006 – On 16 January 2001, CN freight train M31031-15 derailed 26 cars near Mallorytown, Ontario. The derailed cars included two tank cars loaded with propane. The train consisted of 2 head-end locomotives, 149 cars (76 loads and 73 empties), was approximately 9450 feet long and weighed about 11 700 tons. The investigation determined that a combination of the geometricalignment of the track, train marshalling and the buff forces generated during the emergency brake application resulted in a wheel lift derailment.
- R00W0106 – On 16 May 2000, CN freight train E20531-15 derailed 19 cars near Mile 155.0 of the Redditt Subdivision. Four of the derailed cars contained dangerous goods. The train consisted of 2 head-end locomotives, 136 cars (51 loads and 85 empties), was approximately 8800 feet long and weighed about 9440 tons. The investigation determined that, during throttle reduction while in a curve on a descending grade, the train experienced a wheel climb derailment that was a result of high lateral forces created by excessive run-in of the tail-end.