Person overboard
Pilot boat A.P.A. No. 18
Atlantic Ocean, 2 nautical miles east of St. John’s, Newfoundland and Labrador
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
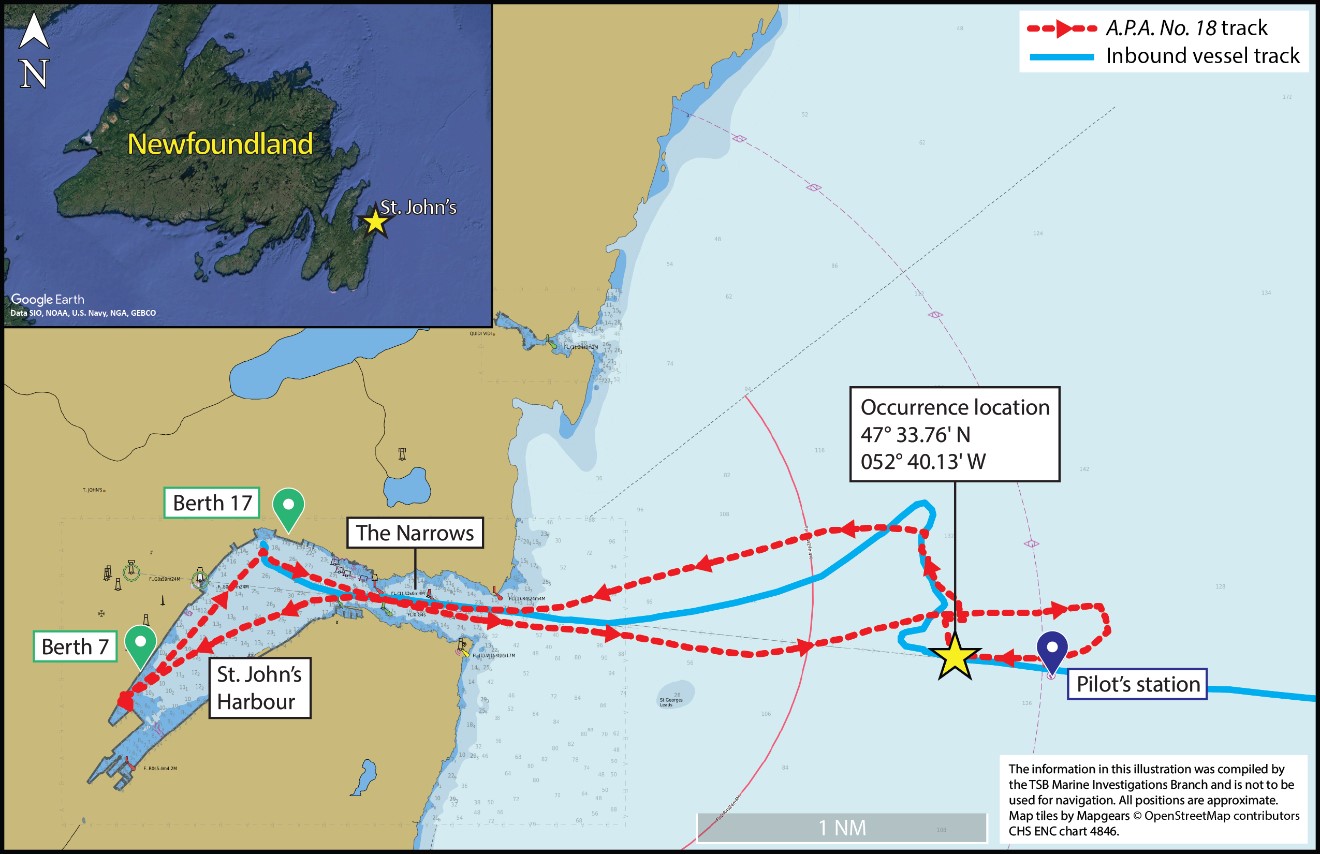
At approximately 2357 Newfoundland Daylight Time on 26 September 2022, shortly after completing a pilot transfer operation to an inbound vessel, the deckhand on the pilot boat A.P.A. No. 18 fell overboard approximately 2 nautical miles east-southeast of the entrance to St. John’s Harbour, Newfoundland and Labrador. Both the master of the pilot boat and crew members on board the inbound vessel attempted to recover the deckhand; the deckhand was recovered by the inbound vessel after being in the water for approximately 20 minutes. The inbound vessel returned to port where the deckhand was pronounced dead.
1.0 Factual information
1.1 Particulars of the vessel
| Name | A.P.A. No. 18 |
|---|---|
| Transport Canada official number | 368950 |
| Port of registry | Halifax |
| Flag | Canada |
| Type | Workboat / Pilot boat |
| Gross tonnage | 50.85 |
| Length overall | 18.78 m |
| Built | 1974 |
| Propulsion | Self-propelled, twin-screw |
| Crew on board | 2 |
| Owner and authorized representative | Atlantic Pilotage Authority |
| Ship manager | Canship Ugland Ltd. |
| MMSI (maritime mobile service identity) | 316007694 |
1.2 Description of the vessel

The A.P.A. No. 18 is a twin-screw, aluminum hull, 18.78 m long pilot boat, built in 1974 (Figure 1) that is used to transport pilots between land and an inbound vessel, or to transport pilots from outbound vessels to land. The vessel is owned by the Atlantic Pilotage Authority (APA), managed by Canship Ugland Ltd. (Canship) and is crewed with 1 masterFootnote 1 and 1 deckhand while conducting pilot transfer operations.
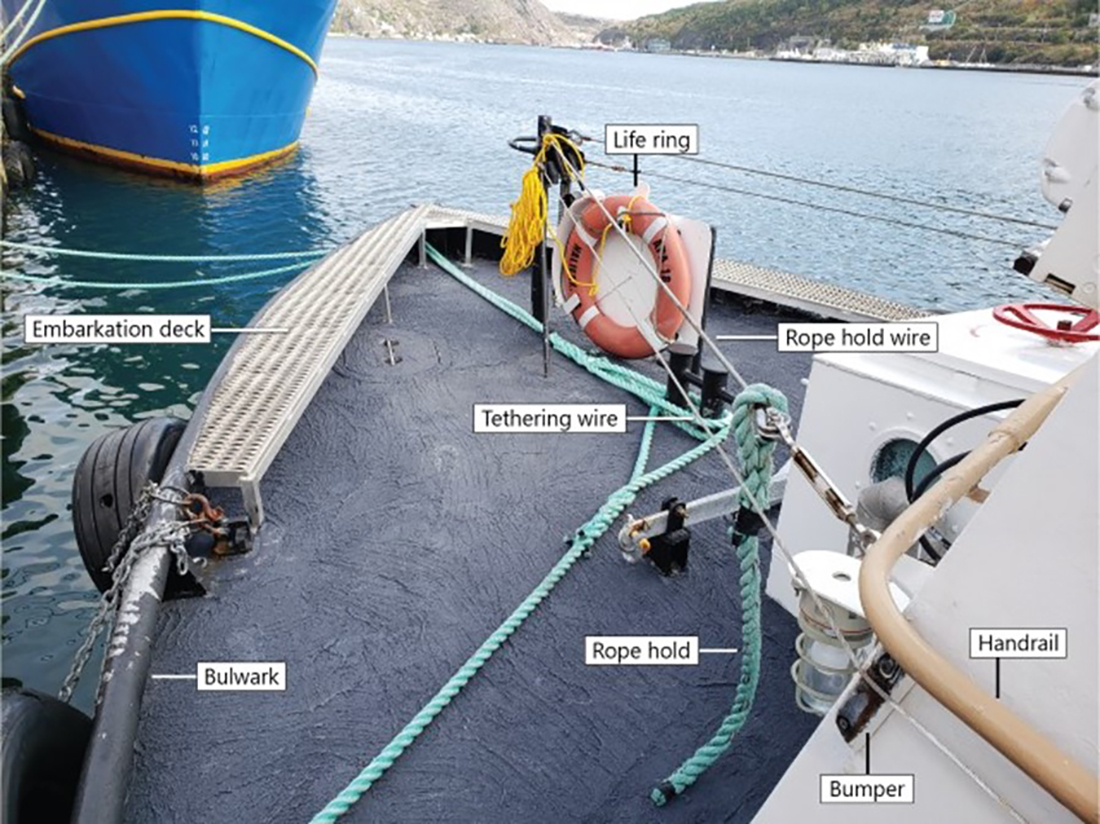
The vessel’s wheelhouse is located forward of amidships and is raised by approximately 1 m from the main deck. Crew members can exit the wheelhouse to the raised outer deck via the wheelhouse aft door or a lower passageway through another door to the aft deck. The conning position is forward in the wheelhouse, slightly to port of amidships. The port and starboard sides of the bow are mostly visible from this vantage point, but there are blind spots from this position. On either side of the raised outer deck are 2 fixed steps to descend to the main deck, with vertical handrails fitted on either side. On the outer main deck, a horizontal handrail runs the length of either side of the wheelhouse, to which several rope holds are attached. The distance from the corner of the wheelhouse to the fixed steps is about 2 m.
Two wires (one from the port side and one from the starboard side) run from the face of the wheelhouse to the bow stanchion, and a sliding rope hold is attached to each wire. These wires and rope holds act as an extension of the handrail that runs along either side of the wheelhouse, and provide a handhold for pilots and crew members who are working on the bow (Figure 2).
At the time of the occurrence, the vessel was fitted with a wire and tether system that crew members secured themselves to with a tether while working on deck. The tethering wires, separate from the rope hold wires, were attached to the bow stanchion and ran the length of either side of the wheelhouse. The wires were fitted hard against rubber bumpers at the forward corners of the wheelhouse and closely to the wheelhouse sides, with less than 0.63 cm between them and the wheelhouse in some places.
The vessel’s bulwarks are about 0.15 m high. On pilot boats it is typical to have flush decks or low bulwarks. The bow has a grated platform on either side that is approximately 0.15 m in height and lies flush with the bulwarks; the platform is about 2 m long and 0.5 m wide and is used as the vessel’s embarkation deck.
The A.P.A. No. 18 is fitted with 3 life rings: 1 on the bow and 1 on either side of the stern. The vessel carries a person-overboard retrieval system and a Jason’s Cradle, and is equipped with a searchlight.
1.3 History of the voyage
On 26 September 2022, the master and 1 crew member (deckhand) of the A.P.A. No. 18 conducted 3 outbound pilot transfers from St. John’s Harbour, Newfoundland and Labrador, each taking approximately 2 hours to complete (at 0700,Footnote 2 1115, and 1930 respectively). At 2300, the master and deckhand began preparing for an inbound pilot transfer operation. At approximately 2312, after conducting engine checks, the A.P.A No. 18 departed Berth 7 with the master and deckhand on board, proceeding to Berth 17 FP (locally known as the finger pier)Footnote 3 to bring the pilot on board.
At around 2320, the A.P.A. No. 18 departed the berth and proceeded on a course toward the pilot station, which is a position approximately 2 nautical miles (NM) east-southeast of The Narrows (Figure 3). While transiting out of St. John’s Harbour, the master of the A.P.A. No. 18, the pilot, and the master of the inbound vessel discussed via very high frequency (VHF) radiotelephone the specifics of the upcoming transfer operation. A plan was established for the pilot boat to approach the inbound vessel on the vessel’s starboard side at a speed of approximately 7 knots.
In preparation for the transfer, the pilot donned an inflatable personal flotation device (PFD) that had an attached automatic identification system (AIS) transmitter with a built-in strobe light-emitting diode (LED). The deckhand donned personal safety equipment which included a safety belt, a tether, and an inflatable PFD that also had an AIS transmitter and built-in strobe LED.Footnote 4
At approximately 2353, when the pilot boat was alongside the inbound vessel with its heading at approximately 270° true (T), the deckhand exited the wheelhouse via the aft door. The deckhand proceeded down the fixed steps and to the bow. The deckhand connected his tether to the vessel’s wire.
At about 2354, the pilot followed the deckhand to the bow. At 2355, the pilot stood on the A.P.A. No. 18’s embarkation deck and made the transfer to the aft deck of the inbound vessel without a pilot ladder. Shortly after, the master of the A.P.A. No. 18 saw the deckhand give a thumbs-up signal, indicating the pilot was safe on board the inbound vessel. The master started pulling the A.P.A. No. 18 away from the inbound vessel, and the deckhand left the bow and headed toward the vessel’s port side. The deckhand disconnected the tether from the wire per common practice, likely at the port corner of the wheelhouse.
The master of the pilot boat did not see the deckhand fall overboard. At about 2357, the master heard yelling from the inbound vessel and looked back to see the deckhand in the water astern of the A.P.A. No. 18. At this time the pilot boat and the inbound vessel were about 2 m apart. The master of the A.P.A. No. 18 immediately stopped the vessel, exited the wheelhouse, and threw a life ring into the water. At about the same time a crew member of the inbound vessel threw a life ring into the water. The master then returned to the wheelhouse, turned the A.P.A. No. 18 to starboard, turned on the searchlight, and proceeded to the deckhand’s location.
Around 2359, the master saw the deckhand near the bow of the pilot boat, stopped the vessel, went on deck, and tried to get a second life ring with a heaving line to the deckhand. The pilot boat drifted from its position and the master lost sight of the deckhand under the bow of the vessel.
In the meantime, the inbound vessel had altered course to return to the deckhand’s location. On 27 September 2022, at around 0002, the inbound vessel located the unresponsive deckhand under the bow of the pilot boat. The pilot boat manoeuvred away from the deckhand and kept the searchlight on him. The inbound vessel manoeuvred closer to the deckhand and its crew members used boat hooks to get hold of the deckhand and bring him along the inbound vessel’s port side working deck. A crew member used a pilot ladder to go over the side of the inbound vessel and put a rope around the deckhand. Once the rope was in place, the crew member ascended onto the inbound vessel’s working deck, and 3 crew members pulled the deckhand out of the water through an opening in the bulwarks. The deckhand was recovered from the water at approximately 0017 wearing an uninflated PFD. The safety belt and tether were not recovered.
Once the deckhand was on board the inbound vessel, first aid was provided, and the inbound vessel proceeded into St. John’s Harbour. At 0045, the A.P.A. No. 18 secured at Berth 7. At 0047, the inbound vessel secured at Berth 17 FP, where an ambulance was waiting to provide medical assistance to the deckhand. The deckhand was taken to hospital by ambulance and pronounced dead.
1.4 Environmental conditions
The weather at the time of the occurrence was mostly overcast, with winds averaging 20 knots from the southwest and maximum gusts up to 25 knots. The air temperature was 14.8 °C and the water temperature was 14.1 °C. Wave heights averaged 1.5 m with a 2.5 m maximum height from the south-southeast. There was light precipitation and visibility was approximately 2 NM.
1.5 Vessel certification
The A.P.A. No. 18 was subject to the Vessel Safety Certificates Regulations and was required to undergo a periodic Transport Canada (TC) inspection for certification every 4 years. TC inspected the vessel on 26 March 2020 and issued an inspection certificate for Near Coastal, Class 2 voyage, which required the vessel to remain within 5 NM from shore. TC also issued a record of safety equipment and a safe manning document (SMD).
According to its SMD, the A.P.A. No.18 was required to have on board a master with a certificate of Master, Limited for a Vessel of Less Than 60 Gross Tonnage and 1 crew member.
1.6 Personnel certification and experience
The master of the A.P.A. No. 18 held a Master Mariner certificate of competency. He had also completed a Marine Emergency Duties (MED) A2 course in 1991 and a refresher course in 2021. The master was employed by Canship and had worked on board the A.P.A. No. 18 for 3 years before the occurrence.
The deckhand held a Fishing Master, Third Class, and Able Seafarer Deck certificates of competency. He had been employed with Canship for approximately 6 months before the occurrence and had worked in the fishing industry for several decades before that.
1.7 Atlantic Pilotage Authority and Canship Ugland Ltd.
The APA is a federal Crown corporation responsible for providing marine pilotage service in the 17 compulsory pilotage areas in Atlantic Canada. A total of 27 pilot boats are used for pilotage services across Atlantic Canada. The APA owns 11 pilot boats, and the remaining pilot boats are provided under contract by commercial operators.
The APA has 3 models for delivering pilot boat services:
- The APA provides and manages both pilot boats and crews.
- A contractor provides and manages both pilot boats and crews.
- The APA owns the pilot boats, and a contractor provides and manages the crew and day-to-day operations.
Canship is a Canadian ship management company located in St. John’s, Newfoundland and Labrador.Footnote 5 Canship is the contractor that provides crew and manages day-to-day operations on board the APA’s 3 pilot boats located in Newfoundland and Labrador.Footnote 6 In addition to the 3 pilot boats, Canship manages and operates multiple large vessels, such as tankers and cargo ships, on the east and west coasts of Canada as well as in northern Europe.
1.7.1 Pilot embarking and disembarking
The transfer of marine pilots at sea is an inherently high-risk activity for both the pilot and crew of the pilot boats. The low bulwarks and the act of transferring personnel from one vessel to another in a dynamic environment presents unique hazards to the pilot and deckhand. In an effort to mitigate these risks, Canship has posted procedures on its pilot boats.Footnote 7 Before conducting a pilot transfer operation, pilot boat deckhands are required to wear a PFD in warmer months or a floater jacket in colder months, and a tether that they must connect to the wire and tether system of the vessel they are working on as soon as they step on deck. Once tethered, the deckhand will go from the wheelhouse to the embarkation deck on the vessel bow and the pilot will follow. The pilot does not wear a tether while embarking or disembarking a vessel.
According to Canship’s procedure, the pilot boat must be alongside the inbound or outbound vessel before the pilot attempts to embark or disembark. When the pilot has only a short distance to climb to embark a vessel, for example when a pilot ladder is not needed, the pilot boat should remain alongside until the pilot is on board, as was the case on the day of the occurrence.
Once the pilot has disembarked from an outbound vessel onto the pilot boat, the pilot boat master should ensure that the pilot and deckhand are safely inside the wheelhouse before pulling away from the outbound vessel’s side.
1.8 Safety management
A safety management system (SMS) is a documented, systematic approach to assessing and managing operational risk, which provides individuals at all levels of an organization with the tools they need to make sound decisions in routine and emergency operations. An effective SMS includes processes, which help to ensure safe practices in vessel operations, a safe working environment, and should also serve to continuously improve the safety management skills of personnel ashore and on board vessels, including preparing for emergencies.
Risk management within an SMS is an ongoing cycle that helps companies and vessel operators identify hazards and assess, mitigate, and follow up on existing and potential risks. One of the objectives of an SMS is to ensure safe operations for a vessel, which can be achieved by assessing all identified risks to a vessel, personnel, and the environment, and to establish appropriate safeguards. In order to be effective, an SMS must be vessel-specific and related to the operations on board. Footnote 8,Footnote 9
The quality of risk management depends on the completeness of hazard identification. The ability to detect and identify hazards depends particularly on the communication of safety-related information between the operational level (master and crew) and the organizational level (management) in an organization. To make this effective, several sources of safety information should be considered, such as previous incidents, hazard reporting, near-miss reporting, debriefing from drills and exercises, occupational health and safety committee minutes, non-compliance reports, inspection and audit reports, and regulatory guidance. A reporting culture is a key component of the safety culture needed for the effective communication of safety information. Footnote 10
The communication of safety information is key to ensure hazards are identified, risks are assessed and mitigated, and procedures are continuously improved upon. Understanding gaps between procedures and work practices is essential and can be achieved by empowering all operational-level employees to communicate these gaps. Footnote 11,Footnote 12, Footnote 13 This process of continuous improvement supports increased communication across hierarchical levels of an organization. When the flow of safety information is affected, then continuous improvement is difficult to achieve in an SMS.
1.8.1 Safety management in the Atlantic Pilotage Authority
The APA has a quality, health, and safety system that is derived from ISO 9001 standards, that shares many, but not all, of the same aspects of an SMS certified according to the International Safety Management (ISM) Code. The APA is not required to have an SMS, and has implemented this combined system.
Following the APA’s combined system, key members of the APA’s management team conduct risk analysis to develop and update programs and procedures for APA operations. Depending on the operating model of the APA vessel, different risk mitigations apply. For example, APA-managed vessels (Halifax vessels) have a robust drill program where person-overboard drills are required to be conducted, recorded, and debriefed. The resulting safety information is integrated into the APA’s system for continuous improvement. Canship-managed vessels (St. John’s vessels) conduct person-overboard drills regularly, and feedback and lessons learned following the emergency drills can be provided to management via the safety committee minutes; however, between January 2022 and September 2022 no feedback on the drills was recorded in the safety committee minutes. Some 13 checklists and forms (the same checklists and forms that are part of Canship’s SMS for pilot boats) are provided to all pilot boats associated with the APA; these checklists and forms must be kept on board.
The APA conducts evaluations of all its vessels and applicable procedures, which consists of an annual inspection of vessels and equipment, and an operational audit of procedures; however, the A.P.A. No. 18’s annual inspection and audit for 2020 were not conducted due to COVID-19 restrictions. The last inspection and audit completed before the occurrence was on 16 September 2021.
1.8.2 Safety management in Canship Ugland Ltd.
Canship is required by regulation to have a certified SMS in place for some operations it manages. For the APA pilot boats that Canship manages, an SMS is not required. The purpose of Canship’s SMS is to safely manage operations. Canship’s SMS has several objectives: to provide shore-based and shipboard managers and employees with practices and procedures to comply with mandatory rules and regulations, to effectively control operations, and to keep necessary records.
The SMS consists of 5 manuals that were last updated in early 2022: the Pilot Boat Operations Manual, the Policy, Quality and Environmental Manual, the Administration Manual, Emergency and Security Procedures Manual, and the Shipboard Safety Manual. Most of these manuals are designed for larger vessels such as tankers or cargo ships, and much of the information is not relevant to the smaller pilot boats managed by the company.
Canship’s SMS indicates that the Pilot Boat Operations Manual, the Policy, Quality and Environmental Manual, and the 13 checklists and forms developed by the APA are the primary Footnote 14 SMS resources for pilot boats managed by Canship. The 13 checklists and forms developed by the APA include templates for masters’ hand-over notes and shipboard safety committee meetings, and safety checklists. Canship’s 3 other manuals are available to the pilot boats, but are considered by crew to be secondary components of the pilot boat SMS. Canship’s SMS is audited internally, which is when crews’ awareness of the system is assessed.
The Pilot Boat Operations Manual puts the onus on masters to implement continuous improvement of the SMS by ensuring the company addresses all suggestions for improvement. The mechanism for masters at the operational level to communicate with the company at the organizational level is through the safety committee and a maintenance defect list. Although the crew members who work on board the A.P.A. No. 18 communicate hazards and incidents among themselves, the investigation determined that hazards relating to factors in this occurrence such as 2-person manning levels, emergency response to person overboard, or fatigue were not communicated to the organizational level via the safety committee, nor were any other reports of these hazards found.
For emergency procedures, procedures for drills and exercises and incident/hazard/near-miss reporting, as well as some on-the-job training, masters must look outside the primary pilot boat SMS manuals. The incident report procedure lists the types of incidents to report and how to report them. In addition, this procedure explains the importance of hazard identification; however, the reporting examples are all severe events. Footnote 15 No examples of hazards or unsafe conditions are listed in this procedure.
1.8.3 Interaction of Atlantic Pilotage Authority and Canship Ugland Ltd. safety management systems
APA pilot boats that are managed by Canship are subject to Canship’s SMS, and so when the APA requires a procedure to be added to its pilot boat operations, the procedure comes into effect through Canship’s SMS. Canship conducts internal audits to oversee its system; the last audit before the occurrence was conducted on 20 October 2021.
The on-the-job training provided by Canship to the crew of the A.P.A. No. 18 originates from APA guidance. The training references some programs that are applicable only to APA-managed vessels. For example, APA’s personal protective equipment program and drill program are referenced in Canship’s on-the-job training; however, these programs do not apply to contracted crew vessels such as the A.P.A. No. 18.
1.9 Procedures, adaptation, and work
Procedures are routinely applied by experienced, trained individuals in the marine industry. Procedures exist to provide standardization and to describe task steps, however, sometimes there can be mismatches between procedures and work practices.Footnote 16,Footnote 17 Mismatches can occur when a procedure is developed without worker input, when procedures from one part of an operation are applied to another, or when the design of the equipment and procedure do not match. A mismatch creates a gap between how work is written into a procedure and how it is applied. This gap creates opportunities for work to be adapted when reconciling multiple goals such as working safely, getting the job done, and complying with regulations.Footnote 18
Adaptations are often judged negatively or seen as the cause of accidents.Footnote 19 However, adaptations are often needed and can offer solutions to making things work in complex environments. Adaptations can be made or develop over time in response to operational needs; for instance, a procedure with too few steps can have steps inserted by workers to perform work more effectively, when a procedure is impractical for the equipment provided the task may be done in a slightly different way, or when a procedure cannot be followed in practice in the operational situation, new steps may be developed.
An absence of familiarization, recurrent training, or routine checking on how work is done in daily operations can increase the likelihood of adaptations occurring without consideration of the adaptations themselves and their impacts. The longer an adapted work practice is applied without incident, the more established the adapted work practice becomes.Footnote 20 Over time, the new and adapted way of working becomes the normal way of working and new crew members can learn these adaptations as the standard practice instead of the actual, written procedure.
A risk in these circumstances is that an adapted practice may have developed without consideration of all the hazards associated with the work and local environment, as well as the mitigations that are designed into a formal procedure to manage those risks. The adapted practice may miss key safety requirements or coordination with other procedures while it still accomplishes the work. These natural, incremental adaptations to accomplish work tasks in complex work environments and conditions can invisibly erode safety margins.Footnote 21
In this occurrence, the deckhands were aware of the need to disconnect in places along the wire and tether system and this was routinely practised.
1.10 Falling overboard
In Canada, falling overboard is one of the leading causes of death in the marine industry. Under the Maritime Occupational Health and Safety Regulations (the MOHS Regulations),when a hazard of drowning exists as a result of work activities, employers are required to provide lifejackets or other flotation devices (that meet the Canadian General Standards Board standard CAN/CGSB-65.7-2007 or equivalent), emergency equipment held in readiness, a written emergency response procedure, and a qualified person ready to intervene.Footnote 22 The A.P.A. No. 18 was subject to the MOHS Regulations.
In addition to the risk of drowning, a person who falls into water that is below 15 °C experiences an initial cold shock response in the first 2 minutes, which can be fatal.Footnote 23 If they survive the cold shock response, cold incapacitationFootnote 24 and exhaustion can quickly set in as they attempt to stay afloat. Exhaustion increases rapidly if the person is not assisted with flotation. PFD use can reduce the adverse consequences of cold shock and increase a person’s chances of survival until help arrives. PFDs do this by keeping the user’s face above the surface of the cold water which reduces the gasp reflex and stops the user from inhaling water. Uninflated PFDs do not assist in flotation.
Risk of hypothermiaFootnote 25 exists in water of temperatures less than or equal to 25 °C and it is significant in water of temperatures less than or equal to 15 °C. Rapid recovery from the water is critical to increasing a person’s chances of survival and can be facilitated by vessels having a person-overboard procedure and a rescue plan in place.
TC is responsible for enforcing the MOHS Regulations. Footnote 26 Some of the ways it does this is through routine visits to workplaces and inspections.
Finding: Other
The A.P.A. No. 18 had not undergone a maritime occupational health and safety inspection by TC in the 5 years before the occurrence.
1.11 Emergency preparedness for person-overboard emergencies
Under the Canada Shipping Act, 2001 (CSA 2001), a vessel’s authorized representative (AR) is required to develop procedures for the safe operation of a vessel and for dealing with emergencies. The AR must also ensure that crew receive safety training.Footnote 27 Under the Marine Personnel Regulations (MPR), crew members are also required to receive on-board familiarization and safety training,Footnote 28 including familiarization with shipboard equipment and operational instructions specific to the vessel. The master is responsible for ensuring that crew knowledge is up to date and that training records are kept on board.
As the AR, the APA requires contracted vessels to complete person-overboard drills every 3 weeks, and written reports of exercises must be posted on the vessel. On the A.P.A. No. 18, person-overboard emergency drills were conducted, personnel were trained, and instructions and equipment for retrieval from the water were available. The person-overboard emergency drills were usually completed inside St. John’s Harbour during the day and sometimes alongside the wharf. The drills were routinely practised with 2 crew members, which is how it would be performed when a pilot was on board. During these emergency drills, the crew would use a person-overboard retrieval system. The A.P.A. No. 18’s records of drills are kept in the vessel’s logbook without a written report.
At the time of the occurrence, a procedure for person overboard was available in Canship’s Emergency and Security Procedures Manual, but that manual was not considered essential by pilot boat crews. The emergency procedure lists specific actions for at least 3 people to effect a recovery, including a master, an officer of the watch, and a person to prepare an emergency boat.
In September 2021, the APA inspected the vessel, which included observing a person-overboard drill. The inspection report concluded that the davit installed on the A.P.A. No. 18 as part of its person-overboard retrieval system was slow and inefficient for recovery, as well as being difficult for 1 person to handle. There were no documented changes as a result of this inspection and the inspection report was not received by Canship management. Further, the crew informally discussed amongst themselves their concerns of facilitating a rescue with 1 person on board the vessel.
1.12 Safe manning
The CSA 2001 indicates that a master should not operate a vessel unless it is manned with sufficient and competent crew for the vessel’s safe operation on its intended voyage, and that it remains so manned throughout the voyage.Footnote 29
TC issues vessels of more than 15 GT with a document containing information on minimum safe manning for the vessel. To apply for a minimum SMD, the vessel’s AR must provide TC with the vessel’s requirements during normal operations and emergency situations. Two TC inspectors independently review the application on the basis of an assessment of the vessel’s requirements using a minimum safe manning evaluation form. The evaluation form contains a matrix, which is used by TC to provide a systematic approach to allocating minimum safe manning requirements to vessels, and reflects the requirements of the MPR, section 207.Footnote 30
TC takes information provided by the AR, such as vessel size, passenger count, engine power, and suggested number of crew members, and applies it to the evaluation form. If both inspectors agree that the minimum number of crew proposed meets regulatory requirements, the SMD is issued. The SMD specifies the minimum number of crew members required on board the vessel, their levels of certification, and a description of the voyages that the vessel is permitted to undertake with that minimum crew complement. An SMD is valid for 5 years, and the AR must contact TC to renew the document before it expires. As part of the renewal process, a TC inspector visits the vessel to verify that its operating conditions have not changed.
In addition to the vessel information provided by the AR, the evaluation form takes into consideration crew requirements for fire, abandon ship, and post-abandonment emergencies. The minimum safe manning level is established from the emergency scenario with the highest number of crew members required and does not consider the number and qualifications of crew members required to safely carry out other vessel operations, such as transfer of personnel. Vessels may be issued several SMDs at the same time for different voyages.
Some vessel requirements identified on the evaluation form are prescribed; i.e., a certain number of crew members are specified by regulations. Other requirements are non-prescribed, meaning the number of crew members is not specified by regulations and is determined by TC based on a number of factors, such as a best practice. These non-prescribed requirements may allow for variability in the minimum number of crew on pilot boats.
According to TC, the minimum number of crew members for pilot boats vary from 1 region to another across the country. For example, in the Atlantic region, most pilot boats have a safe manning level of 2 crew members, whereas in the Laurentian region pilot boats have a safe manning level of 3.
APA uses SMDs to establish crewing levels and all of the pilot vessels owned by the APA are crewed only to their minimum safe manning level, as is common practice in the marine industry. The A.P.A. No. 18’s latest SMD was issued in 2020 (Table 2); at that time, TC’s evaluation form included the following emergency scenarios: fire, abandon ship, and post-abandonment.
| Year safe manning document issued | 4-person safe manning document issued | 2-person safe manning document issued |
|---|---|---|
| 2008 | 4 persons (NC2 voyage)* | No document issued |
| 2011 | 4 persons (NC1 voyage)** | 2-person (NC2, limited to servicing vessels at the Placentia Bay outer pilot station) |
| 2015 | 4 persons (NC1 voyage) | 2-person (NC2, limited to servicing vessels at the Placentia Bay outer pilot station) |
| 2016 | No document issued | 2 crew (NC2, limited to HTIII*** no further than 20 NM from shore) |
| 2018 | No document issued | 2 crew (NC2, limited to St. John’s Harbour and approaches, not more than 5 NM offshore) |
| 2020 | No document issued | 2 crew (NC2, limited to HTIII no further than 20 NM from shore) |
* Near Coastal voyage, Class 2, as defined in the Marine Personnel Regulations (as amended 01 July 2007).
** Near Coastal voyage, Class 1, as defined in the Marine Personnel Regulations (as amended 01 July 2007).
*** Home-trade voyage, Class 3 (HTIII), as defined in the Home-Trade and Minor Waters Voyages Regulations (as amended 01 July 2007).
In July 2022, a TC inspector assigned to issue an SMD for one of the A.P.A. No. 18’s sister ships challenged the issuance of the SMD through TC’s regional structure. The challenge concerned the facilitation of a rescue of an unconscious casualty in the water with only 2 crew members. According to TC, this challenge did not result in a change to the SMD to require more personnel, in part because a rescue conducted in this manner was a non-prescribed requirement in TC’s SMD evaluation form. Late in 2022, TC updated the evaluation form to add a non-prescribed requirement, which requires ARs to provide details on how a person-overboard emergency would be dealt with. These details are now part of the minimum safe manning evaluation for all vessels.
1.13 Post-occurrence drug and alcohol testing
Testing for alcohol and drug use in federally regulated workplaces is guided by human rights legislation, labour standards, collective agreements and decisions from labor arbitrators, administrative tribunals, and court proceedings where the overall effort in these decisions is to balance two competing objectives: preserving individuals’ human and privacy rights and ensuring employee and public safety.Footnote 31 Current Canadian marine safety regulations do not require systematic drug and alcohol testing, for example, as part of monitoring of the safety of marine operations or following a marine accident or incident.Footnote 32
Canship’s Drug and Alcohol PolicyFootnote 33 requires a drug and alcohol test following any incident which is reportable under the Transportation Safety Board Regulations. Post-mortem toxicology testing was carried out on the deckhand by Newfoundland and Labrador’s Office of the Chief Medical Examiner as part of the chief medical examiner’s protocol; however, following the occurrence, no testing was conducted on other APA or Canship personnel involved in the occurrence.
Finding: Other
There is no mandatory post-occurrence drug and alcohol testing in the marine industry for Canadian crews involved in occurrences.
1.14 Fatigue
Sleep-related fatigue is widely reported in marine operations, and results from insufficient good-quality sleep, which can come from lack of sleep and inconsistent sleep times.Footnote 34 The risk of sleep-related fatigue is increased by long shift durations, standby duties, and sleep opportunity on mandatory rest period during the daytime. With excessive levels of fatigue almost all aspects of human performance are degraded, including those associated with vigilance, reaction time, and problem solving. The risks associated with sleep-related fatigue must be effectively managed in marine operations, like other hazards. Fatigue risk management requires a proactive approach by organizations that includes not only compliance with regulations (which can only ever mandate hours of rest, not hours of sleep) but also mariner education and awareness. For sleep to be restorative, it should occur at night in a period of at least 7, and up to 9, continuous hours.Footnote 35,Footnote 36
Regulations that set out duty time limitations and minimum rest requirements are basic fatigue mitigations. These regulations establish work time limits and provide employees with the opportunity to obtain sleep; however, these regulations do not (and cannot) ensure that the individual is well rested. Under the Marine Personnel Regulations, masters on pilot boats like the A.P.A. No. 18 are required to ensure that the master and every crew member has at least 6 consecutive hours of rest in every 24-hour period, and at least 16 hours of rest in every 48-hour period. The regulations also stipulate not more than 18 hours but not less than 6 hours can elapse between the end of a rest period and the beginning of the next rest period.Footnote 37,Footnote 38
1.14.1 Fatigue in A.P.A. No. 18 operations
The work schedule of the crew members who work on board the A.P.A. No. 18, including the master involved in this occurrence, follows 1 of 2 formats:
- 7 days on duty and 14 days off, with 24-hour availability while on duty; or
- 14 days on duty and 7 days off, with 24-hour availability while on duty.
Masters monitor tentative pilot transfer requests through the APA’s mobile application. Masters generally receive 12 hours’ notice for inbound transfers and 4 hours’ notice for outbound transfers; the assignment time is subject to change. When the timing of the assignment is firm, APA dispatch will relay the assignment to the master. Masters manage work/rest hours by recording hours worked in a spreadsheet throughout the day. When hours of work appear to be close to the 18-hour limitation, the master will call in a relief crew member or ensure a rest period is available.
Opportunities for rest occur as a regular part of the A.P.A. No. 18’s daily operations, where crew members can be released from the vessel several times during a 24-hour period. Crew members are required to return to the vessel within 15 minutes of being called while on duty. This irregular and unpredictable work schedule can cause circadian rhythm effects, which have been shown to contribute to fatigue.Footnote 39,Footnote 40 Specifically, circadian rhythm desynchronization causing fatigue can occur with individuals working irregular shifts, especially with shifts of more than 8 hours. Shiftwork-related fatigue has significant risk factors, and split shifts (i.e., work-rest-work-off) can be particularly fatigue-inducing. Working 7 days on duty can allow fatigue risk factors to develop, and working 14 days on duty allows more time for fatigue risk factors to develop and greater magnitude of fatigue in terms of acute sleep disruption, chronic sleep disruption, continuous or prolonged wakefulness, and circadian rhythm effects.
The master and deckhand involved in the occurrence had not undergone training on fatigue awareness or fatigue management, nor were they required to by regulation.
The master involved in this occurrence generally worked a shift schedule of 7 days on duty and 14 days off. He worked 2 extra days before the occurrence to fill in for the vessel’s other master before the start of his week-long shift. The occurrence voyage began at the end of the master’s second day of filling in.
The TSB collected the hours of work and rest periods for the deckhand and was able to estimate his hours of sleep in the 6 days preceding the occurrence. The deckhand’s regular schedule was 7 days on followed by 14 days off, and the occurrence voyage took place on the last day of the deckhand’s 1-week shift. At the time of the occurrence, the deckhand was on day 7 of a 7-day shift and had been awake continuously for 18 hours, including during the regulated rest period of 7.5 hours, which was taken away from the vessel. The TSB’s analysisFootnote 41 identified that the deckhand was subject to the following fatigue risk factors:
- An acute sleep disruption of 4 hours over a period of 72 hours.Footnote 42
- A chronic sleep disruption with a sleep debt of 7.5 hours over a period of 120 hours.Footnote 43
- Continuous wakefulness totaling 18 hours on the day of the occurrence.
- Circadian rhythm desynchronization as a result of variable and unpredictable work schedules resulting from a 24-hours-a-day / 7-days-a-week availability, periods of work and rest scattered through a shift with no pattern, and early and late work tasks.
- A circadian rhythm low, given that the accident happened near midnight, which is during the circadian rhythm trough.Footnote 44
Finding: Other
The deckhand was subject to multiple fatigue risk factors such as acute sleep disruption, chronic sleep disruption, continuous wakefulness, circadian rhythm effects, and likely was fatigued at the time of the occurrence.
1.15 Safety equipment
1.15.1 Wire and tether system
At the time of the occurrence, the wire and tether system on board the A.P.A. No. 18 consisted of a wire fitted to the vessel, a belt worn by a crew member, and a single tether that connected the crew member’s belt to the wire. This system was put in place by APA and Canship to mitigate the risk of crew members falling into the water while conducting work on the outer deck of the pilot boat.
The wires were made of stainless steel, approximately 0.5 inches in diameter. One end of each wire was attached to the bow stanchion with a turnbuckle; the other end was attached with a hard eye connector just forward of the fixed steps.
The safety belt was made of 7.6 cm yellow web nylon polyester and had a tongue buckle that could be adjusted. A D-ring was fitted on the back of the belt, which clipped to one end of an approximately 60 cm tether made of yellow web nylon. The other end of the tether could be connected to the wire. The tethers on the A.P.A. No. 18 were used by the multiple crew members who work on the vessel.
1.15.2 Person-overboard retrieval system
The A.P.A. No. 18 has a person-overboard retrieval system consisting of a long metal pole with an adjustable loop at 1 end. The pole can be attached to a block and tackle lifting arm (davit) that is permanently attached to the starboard side of the vessel around amidships. The pole and lifting tackle can be used together or separately to retrieve a conscious or an unconscious person from the water. The size of the adjustable loop can be controlled by the rescuer. It is possible for a single person to operate the retrieval system provided there is another person available to manoeuvre the vessel.
1.15.3 Personal flotation devices
In Canada, lifejackets and PFDs come in many shapes, sizes, and colours. Although the terms “lifejacket” and “PFD” are often used interchangeably in Canada, a PFD is not considered to be a lifejacket.Footnote 45 There are multiple manufacturers and designs of PFDs and each manufacturer has specific instructions for the maintenance and servicing of its products, which can vary depending on the design. PFDs can be inherently buoyant or inflatable. Inherently buoyant PFDs have buoyancy regardless of when or how they are used and require very little maintenance compared to inflatable PFDs. Inflatable PFDs are less restrictive than inherently buoyant PFDs, and are more likely to be used for this reason. Inflatable PFDs require more maintenance,Footnote 46 which must be carried out according to manufacturer’s instructions for the PFDs to function correctly.
Vessel lifesaving devices, such as life rafts, are required to be maintained by an accredited third party.Footnote 47 In contrast, inflatable PFDs do not have regulated service requirements, although vessel owners may choose to send PFDs to a third party for servicing. Manufacturers sometimes choose to accredit third parties to service their PFDs.
The United States Coast Guard issued a Marine Safety Alert in 2016,Footnote 48 and TC issued a Ship Safety Bulletin in 2019,Footnote 49 highlighting incidents in which improper maintenance affected PFD inflation, resulting in fatalities. These safety messages were issued to remind users of the importance of maintaining inflatable PFDs in accordance with manufacturer’s instructions.
The A.P.A. No. 18 was required to carry, and did carry, enough lifejackets on board for the maximum capacity of the crew.Footnote 50 However, the work conducted by deckhands on the A.P.A. No. 18’s deck was identified by management as a risk of drowning, so inflatable PFDs were worn by crew members when they worked on deck.
1.15.4 Personal flotation device worn in the occurrence
Footnote 51
The occurrence PFD (Figure 4) was an inflatable collar type, red on the outside and yellow when inflated, had 2 heavy-duty D-rings for tethers, and had a person-overboard locating device attached.Footnote 52 The PFD was designed to be used in an offshore environment and had 38 pounds of buoyancy when inflated. It was designed to inflate using a 2-part inflator cap and inflator body system; when the complete assembly was installed, the inflator body with attached CO2 cartridge was designed to fit within the PFD bladder, with the cap on the outside and visible through an inspection window.
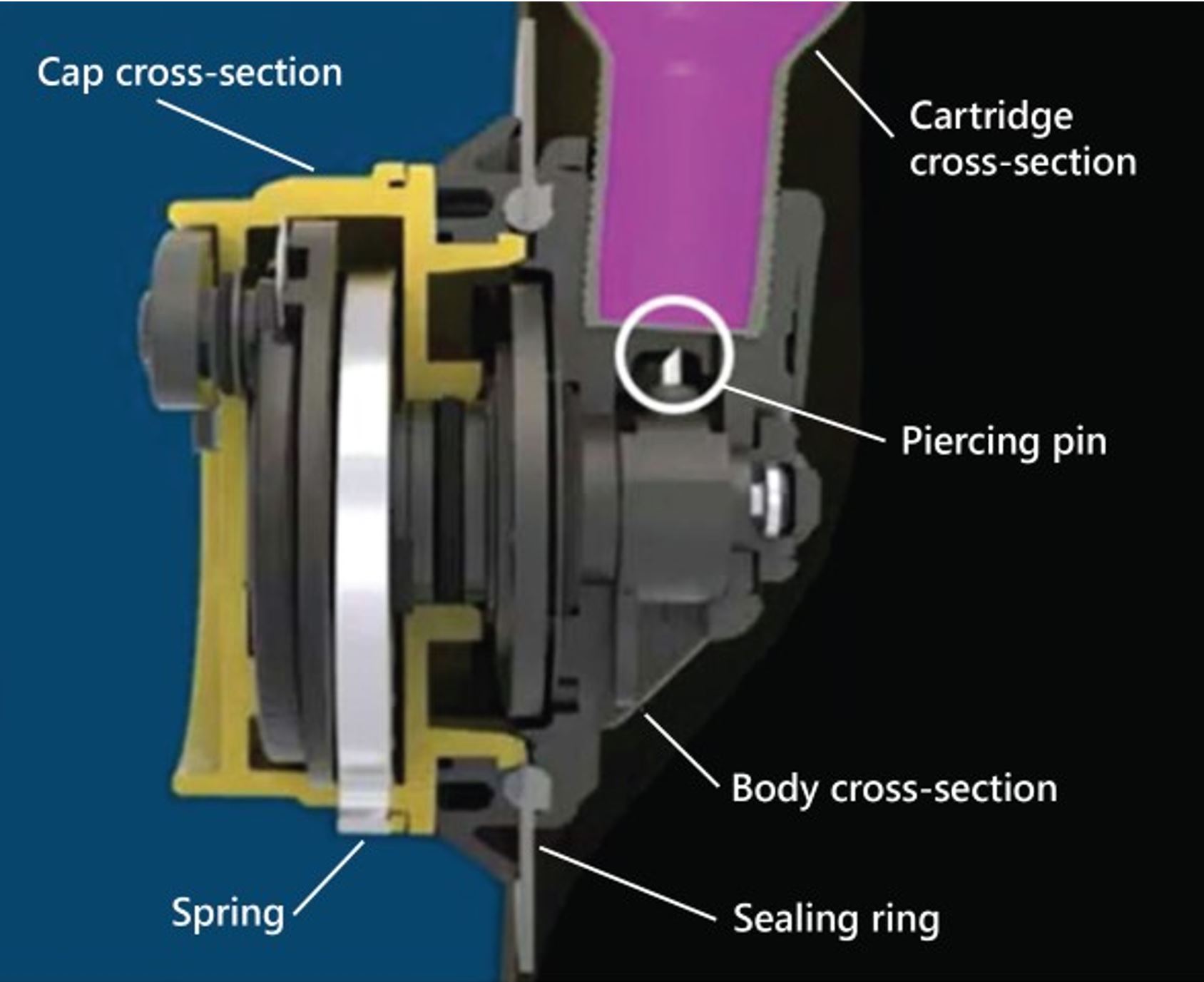
The cap contains an inflation activation mechanism that can be initiated in 2 ways: manual activation using a pull tab, or automatic hydrostatic activation. When the cap is activated, the energy stored in the cap’s coiled spring generates a rotational force that is transferred to the piercing mechanism in the inflator body. Through a cam action, this rotation causes the piercing pin to be driven through the top of the CO2 cartridge and then withdrawn (Figure 5). Once the cartridge is pierced, CO2 gas is released into the bladder of the PFD, inflating it. Inflatable PFDs always have an oral inflation tube in case the CO2 inflation system fails or the bladder requires a top-up of air.
In order for the occurrence inflatable PFD to function, and for the bladder to remain inflated once filled, the cap and body must be securely mated, sandwiching a soft silicone ring in the bladder wall which serves as a gasket. This mating provides the bladder with a gas-tight seal. If this is not done correctly, the bladder will not retain CO2 or air, and the PFD will not inflate.
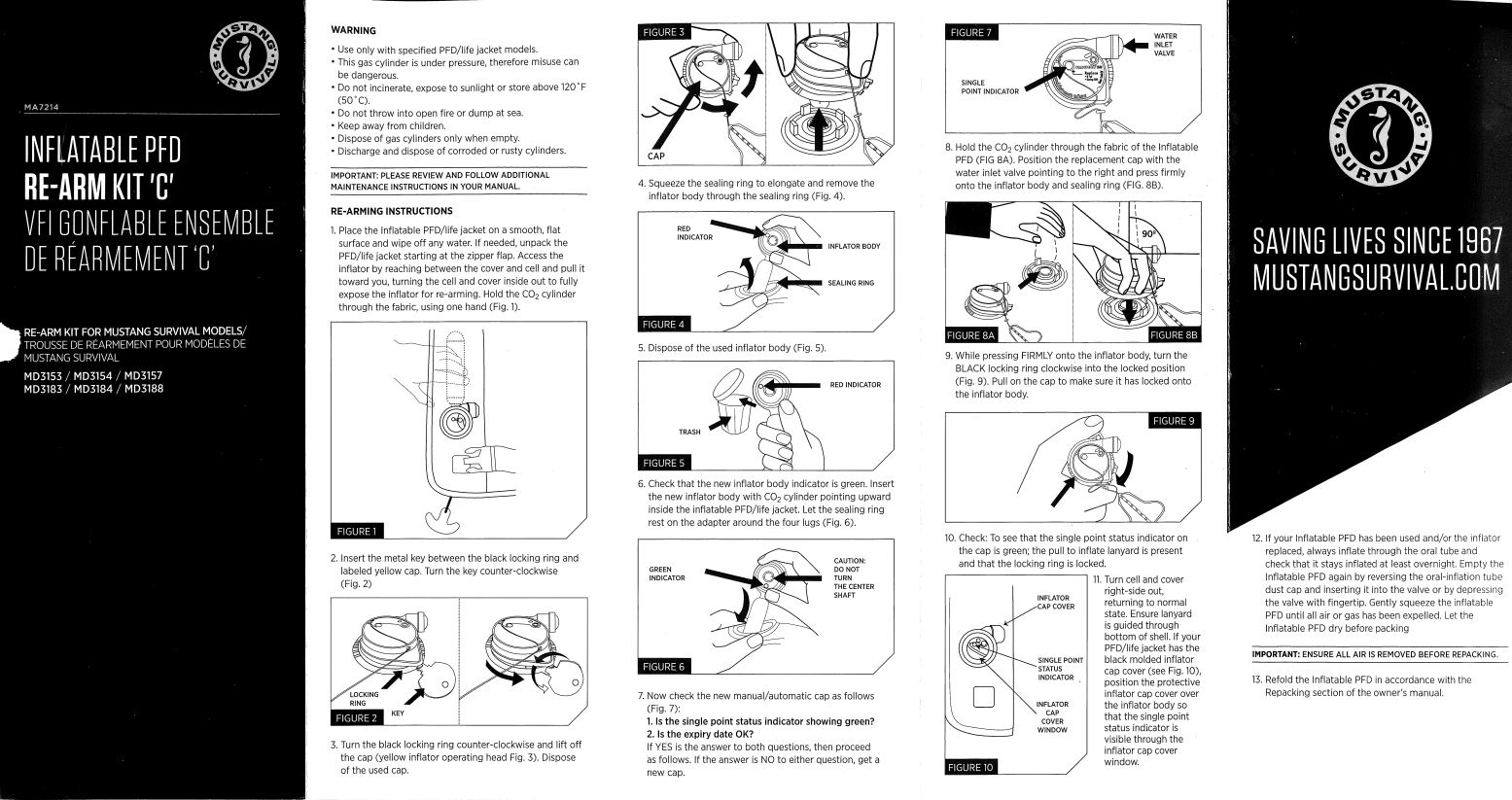
The manufacturer for the occurrence PFD provides an owner’s manual in which there is a checklist for readiness inspections, pre-use inspections, and maintenance instructions for 6-month and 1-year intervals (Appendix A). The owner’s manual also has specific instructions on rearming and repacking the PFD which require the PFD to be rearmed every 5 years (per expiry of the inflator system) or after inflation.
Rearming is the process of changing out the inflator parts within the PFD bladder, and a rearm kit from the manufacturer must be used. The rearm kit also includes a set of detailed instructions for rearming the PFD (Appendix B).
All inspections, maintenance, rearming, and repacking can be done by the user or a third party, with the exception of the pre-use inspection, which must be done by the intended user. The owner’s manual indicates that users are responsible for becoming familiar with the use of their PFD; several suggested methods are activating the CO2 inflation system, rearming the CO2 inflation system, and using the oral inflator tube.Footnote 53
The occurrence PFD was shared among crew who worked on board the A.P.A. No. 18. Canship addressed the care and maintenance of PFDs in use on pilot boats by requiring that they be inspected by the master at each change of command and serviced once a year by a third-party service provider. Although Canship policy required personal protective equipment be maintained according to manufacturer’s instructions, the manufacturer’s recommended semi-annual inflation tests and pre-use inspections by the end user were not described in the company policy.
The occurrence PFD was serviced by a third party on 01 April 2022. The servicing included a rearming, inspection, and repacking in accordance with the third party’s Generic Inflatable LifeJacket Service Checklist (the generic checklist). The generic checklist was developed by the third party based on training and material received from Crew Saver, another PFD manufacturer with whom the third party is trained and certified. The generic checklist was developed to ensure important steps were not missed; it leads technicians through the servicing of a variety of inflatable PFDs and includes a leak test, inspection of components, inspection of the general condition, repairs, and repacking. The generic checklist was completed while servicing the occurrence PFD.
Some of the steps in Mustang’s rearming and repacking instructions for its PFDs differ from the generic checklist developed by the third party. Most notably, the air-leak test conducted by the third party was 1 hour long, whereas Mustang’s rearming and repacking instructions indicate the test should be conducted overnight. As well, the generic checklist did not give the same level of detail as the manufacturer’s rearming and repacking instructions. The third party had access to Mustang’s rearming and repacking instructions but rarely referenced them. The third party was not a certified service provider for Mustang PFDs, nor were they required to be to service that manufacturer’s products.
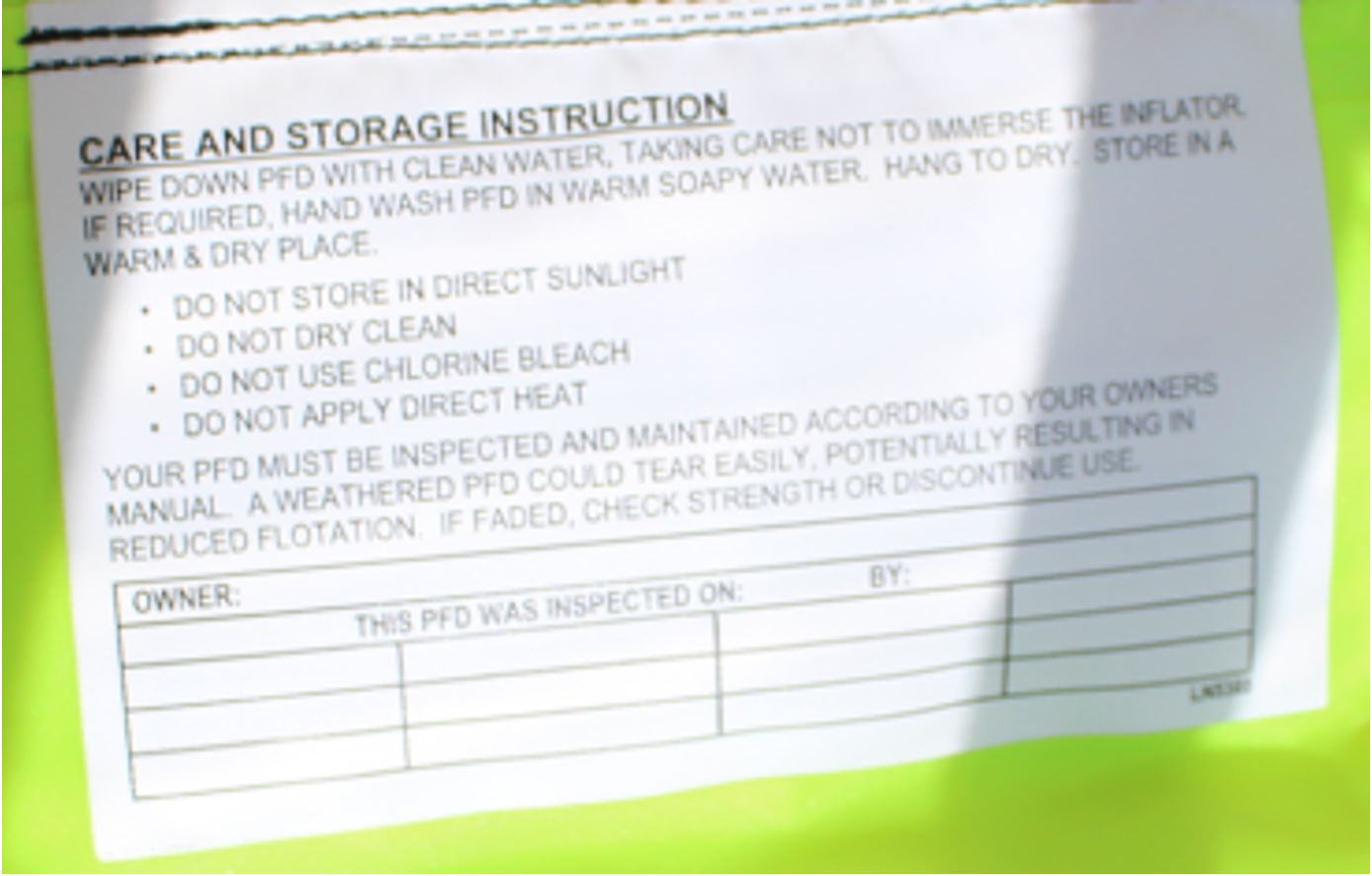
The pilot boat masters have a safety checklistFootnote 54 to use each time they inspect the safety equipment on board their vessels. This checklist is to be completed at every change of command. The PFD inspection requires users to test each person-overboard locating device and strobe LED, and to inspect the cleanliness and overall condition of each PFD. The shared PFDs on board the A.P.A. No. 18 were inspected on 16 September 2022 and 25 September 2022 and the inspections were recorded in the vessel safety checklist. The record of inspection on the care and storage label (Figure 6) inside the occurrence PFD was blank.Footnote 55
1.15.5 Testing by the TSB
Following the occurrence, the PFD was brought to the TSB Engineering Laboratory in Ottawa, Ontario, for a detailed visual inspection, examination, and testing. The occurrence PFD was received in an uninflated condition, with the bladder slightly visible on the lower left side, and the rest of the zipper fastened. The initial visual inspection noted the PFD did not exhibit deterioration such as broken hardware, detached webbing, or rotten structural components that could diminish its performance.
Finding: Other
The manual pull tab on the occurrence PFD was tucked in where it could not be accessed by the user.
During the examination of the occurrence PFD, the expiry date noted on the cap was 2027, and there had been an initial activation of the inflator cap when the water met the water-sensitive element, but the inflator body did not activate. This allowed the inflation activation mechanism inside the inflator cap to rotate. However, the mating gear on the inflator body did not engage and the piercing pin did not move or puncture the CO2 cartridge. The examination and testing determined that the cap and body were unmated. The cap activated and the body did not, indicating that the cap and body were separated at some point prior to the occurrence and not as a result of recovery efforts. Because the inflator cap and inflator body were not mated, the PFD bladder was not sealed, which prevented the PFD from inflating. Further visual inspection, as required by the manufacturer’s instructions for pre-use inspection, would not have detected the separation of the inflator cap and body.
The TSB laboratory conducted testing under various conditions to assess whether it was possible to rearm a PFD, perform an inflation test, and subsequently have the cap and body become unmated during repacking of the PFD. The testing revealed that it was possible to recreate this scenario; however, it could not be done if the manufacturer’s instructions for rearming and repacking were followed.
The attached AIS transmitter functioned as expected during testing.
1.16 Previous occurrences
M19A0090 (oyster boat) – On 08 April 2019, an unnamed and unregistered oyster boat, with 3 people on board, capsized 0.5 NM west of Bayfield, Nova Scotia. Only 1 crew member survived. The investigation revealed a that a PFD used in the occurrence did not inflate due to maintenance not being conducted according to the manufacturer’s instructions.
The TSB has also investigated several occurrences where it was found that crews experienced person-overboard emergencies without adequate emergency preparedness and manning levels to successfully conduct a rescue from the water,Footnote 56 as well as occurrences that highlighted the risks associated with minimum safe manning levels not being sufficient to carry out emergency duties.Footnote 57
Previous TSB investigations have found examples of adaptations to safe work practices that often result in lowered margins of safety.Footnote 58
1.17 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer.
Fatigue management in rail, marine, and air transportation is a Watchlist 2022 issue.
In the marine industry, fatigue is linked to the intensive nature of the business: long and irregular hours of work over extended periods, brief or interrupted sleep, rapidly rotating shifts, high workload, and social isolation. Enforcement of hours-of-work regulations on domestic vessels has been problematic. A strong work ethic, labour shortages, and economic imperatives in the marine industry may also encourage individuals to work while fatigued because of a real or perceived obligation to do so. This makes it more difficult for fatigue to be recognized as a problem and for appropriate action to be taken.
Following an occurrence on 13 October 2016 in which the tug Nathan E. Stewart and the tank barge DBL 55 went aground after the watchkeeper on the bridge, who was fatigued, fell asleep,Footnote 59 the Board made 2 recommendations related to fatigue. In the first, the Board recommended that
the Department of Transport require that watchkeepers whose work and rest periods are regulated by the Marine Personnel Regulations receive practical fatigue education and awareness training in order to help identify and prevent the risks of fatigue.
TSB Recommendation M18-01
In the second, the Board recommended that
the Department of Transport require vessel owners whose watchkeepers' work and rest periods are regulated by the Marine Personnel Regulations to implement a comprehensive fatigue management plan tailored specifically for their operation, to reduce the risk of fatigue.
TSB Recommendation M18-02
In this 2016 occurrence, both recommendations were aimed at managing fatigue in watchkeepers.
In response to these recommendations, TC implemented a 5-year Fatigue Action Plan to address fatigue among seafarers. TC also proposed amendments to the MPR. However, the publication of the new MPR in the Canada Gazette, Part I has been significantly delayed. In February 2024, TC’s response to Recommendation M18-01 was assessed as Satisfactory in Part, and TC’s response to Recommendation M18-02 was assessed as Unsatisfactory.
In the occurrence involving the A.P.A. No. 18, the work/rest provisions in the MPR applied; however, there is no requirement in the regulations for companies to have comprehensive fatigue awareness training or a fatigue management plan.
Fatigue has been identified in previous TSB reports as a contributing factor to accidents, and the presence of fatigue risk factors in this occurrence demonstrates that fatigue persists as an issue within the marine industry.
ACTION REQUIRED Fatigue management in marine transportation will remain on the Watchlist until the following actions are taken:
|
Safety management in rail, air, and marine transportation is a Watchlist 2022 issue.
To date, only Canadian vessels that operate on international voyages and are subject to Chapter IX of the International Convention for the Safety of Life at Sea (SOLAS) must comply with the existing Safety Management Regulations. These regulations do not apply to over 99% of domestic commercial vessels (referred to as non-convention vessels), although a recent “tiered” proposal by TC would expand their applicability. However, even when operators do have safety management processes in place, they are not always able to demonstrate that hazards are being identified nor that effective risk-mitigation measures are being implemented.
Safety management has been on the TSB Watchlist since 2010, and the TSB has investigated many occurrences where it was found that safety management processes were weak or not used.
Since 2004, the TSB has put forward recommendations calling on TC to implement regulations requiring all commercial operators in the marine industry to have formal safety management processes, and effectively oversee these processes (TSB recommendations M04-01 and M17-02). In response, TC proposed the Marine Safety Management System Regulations that will expand formal SMS requirements. The proposed regulations are expected to come into force in 2024.
In this occurrence, although the APA’s combined system applied in part to the A.P.A. No. 18, and Canship’s SMS was in place, many hazards related to routine tasks associated with pilot boat operations were unmitigated. This occurrence demonstrates that issues with safety management persist in the marine industry.
ACTION REQUIRED Safety management will remain on the Watchlist for the air and marine transportation sectors until
|
1.18 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP089/2022 – Inflatable PFD examination
- LP128/2022– Analysis of WamBlee distress alert device
2.0 Analysis
Just before midnight on 26 September 2022, the deckhand working on the pilot boat A.P.A. No. 18 fell overboard. After approximately 20 minutes in the water, the deckhand was recovered and brought to port, where he was pronounced dead. This analysis will examine adaptation of work practices, emergency response, personal flotation devices (PFDs), and the roles of Canship Ugland Ltd. (Canship) and the Atlantic Pilotage Authority (APA) in managing safety for pilot vessels.
2.1 Wire and tether system and necessary adaptations
The transfer of marine pilots at sea is an inherently high-risk activity for personnel working on outer decks. APA and Canship recognized the risk of going overboard while engaged in this activity and implemented mitigation measures to reduce that risk. To reduce the risk of going overboard, there is a procedure for embarking and disembarking pilots. According to the pilot embarking/disembarking procedure, deckhands must connect their tethers to the wire as soon as they step on deck.
This procedure was in place, posted on board the A.P.A. No. 18, and training on how to use the wire and tether system was provided to all deckhands who worked on the vessel. However, because of the wire and tether system’s design and the way it was installed, the deckhands could not use it as intended by procedure. The wire was accessible to deckhands only after they descended the fixed stairs aft of the wheelhouse instead of when they first stepped on deck; from there the wire was fitted closely along the wheelhouse sides and hard against the wheelhouse forward corners such that the single tether used by the deckhands could not slide continuously from the stairs to the bow. These barriers required the deckhands to descend and ascend the stairs untethered, slide the tether along a section of wire where the tether clip head was wider than the space between the wire and the wheelhouse, and disconnect and reconnect around the wheelhouse corner when going out to and returning from the bow during a pilot transfer.
Disconnecting and reconnecting the tether was an adaptation used frequently by deckhands on the A.P.A. No. 18. Because it was impossible to connect the tether to the wire as soon as they stepped on deck, and it was impossible to have the tether continuously connected to the wire, over time the deckhands adapted the procedure to use the handrail instead of connecting to the wire as they stepped on deck and moved to the wheelhouse corner.
Formal procedures frequently have to be adapted at the operational level to make practices work in real life, given local conditions and designs. Adaptations like those used in this occurrence take place because people are trying to accomplish their work while following the procedures. When adaptations develop, there is a risk that associated hazards have not been identified and mitigated. Situations like this demonstrate the importance of an SMS that supports the recognition and communication of operational safety information to management for continuous improvement.
On the night of the occurrence the deckhand working on board the A.P.A. No. 18 was observed with his tether connected to the wire and tether system as he moved toward the bow of the vessel. Once the pilot transfer was completed to the inbound vessel, the deckhand signalled to the master that everything was okay. He then proceeded toward the wheelhouse, disconnecting his tether from the wire likely at the port corner of the wheelhouse as was the usual practice.
The investigation could not determine the exact reason why the deckhand fell overboard. However, given there was no evidence of the wire being broken or damaged, the investigation determined that the deckhand was not tethered to the wire along the port side of the wheelhouse when he fell overboard.
Findings as to causes and contributing factors
The design of the wire and tether system and the way it was installed on board the A.P.A. No. 18 prevented the deckhands from being continuously connected to the wire as they moved between the fixed stairs and bow of the vessel.
The wire and tether system’s design and installation necessitated an adapted practice of disconnecting the tether from the wire while transitioning from the side to the front of the wheelhouse, which contributed to the occurrence deckhand being untethered and subsequently falling overboard.
2.2 Emergency preparedness and safe manning
The success of any emergency operation on board a vessel depends to a great extent on whether there are a sufficient number of crew members with the appropriate qualifications to perform the required tasks. When a vessel has 2 crew members, many emergencies can result in only 1 crew member being available to effect emergency response. For example, when 1 of 2 crew members falls overboard, the remaining crew member is the only person available to effect a rescue while also being responsible for the operation and safety of the vessel. This emergency scenario is compounded by the fact that the likelihood of survival for a person immersed in cold water decreases when retrieval from the water is delayed.
To ensure a timely response to emergencies, a vessel’s on-board level of emergency preparedness needs to be considered. Having an emergency response plan, conducting regular drills and training, considering the design of a vessel in emergency response, and carrying appropriate lifesaving equipment are steps to increase the on-board level of emergency preparedness.
In order to recover a person from the water, a vessel must maintain a position close to the person. When a vessel is stopped, it will move with the sea at a different rate than the person in the water, which means that the vessel must reposition frequently and be actively navigated to maintain a position close to the person in the water. At the same time, the retrieval equipment must be used to remove the person from the water. The wheelhouse of the A.P.A. No. 18 is approximately 2 m from the retrieval equipment. In addition, the person navigating the A.P.A. No. 18 cannot see the water close to the vessel; therefore, they either need direction from a spotter or they must leave the conning position to verify the position of the person in the water. It is therefore unlikely that 1 person would be able to carry out a rescue.
Masters and crew members who worked on board the A.P.A. No. 18 were required to, and often did, conduct person-overboard drills. The drills were completed alongside the wharf at St. John’s Harbour, or on the calm waters of the harbour, and always during the day; these settings did not reflect the usual environment where a person-overboard emergency was likely to take place. The drills were performed with a deckhand available to assist; consequently, the drills did not reveal that a single person could not manoeuvre the vessel and rescue an unconscious person from the water. The A.P.A. No. 18 had a person-overboard checklist that described roles for at least 3 personnel and was therefore not realistic for or relevant to the A.P.A. No. 18 operations and design. The person-overboard checklist was also in 1 of Canship’s SMS manuals that the crew considered to be secondary for pilot vessel operations. This deficiency was not detected in any of the drills or exercises conducted.
The A.P.A. No. 18 was equipped with a person-overboard retrieval system that included a davit, as well as several life rings, and a Jason’s Cradle for retrieving persons from the water. Although an inspection conducted by the APA in September 2021 revealed that the davit was not ideal for a timely recovery, nor for use by 1 person, no changes to the vessel were made.
Previous TSB investigationsFootnote 60 have found a link between lower levels of emergency preparedness and difficulty recovering persons from the water.
Finding as to causes and contributing factors
The design of the vessel combined with its level of emergency preparedness made it practically impossible for the master alone to retrieve the deckhand from the water. Consequently, the deckhand was immersed in cold water for a prolonged period of time.
A vessel’s on-board level of emergency preparedness is in part determined by having a sufficient number of crew to use the equipment available. However, authorized representatives (AR) frequently crew vessels in accordance with minimum safe manning levels. Therefore, minimum safe manning documents (SMDs) can impact the fundamental safety of a vessel and its crew.
When issuing an SMD, Transport Canada (TC) determines a vessel’s minimum complement in accordance with the requirements of the Marine Personnel Regulations (MPR); this minimum complement does not consider that additional crew may be needed depending on the vessel’s operations, and TC expects that ARs will augment the crew as needed. Additionally, the safe manning criteria in the evaluation form used by TC for determining a vessel’s minimum safe manning level did not take into account person overboard or incapacitation emergencies, so these scenarios where not considered when TC evaluated the safe manning levels for the A.P.A. No. 18 and issued its SMD. Consequently, the SMD on board the A.P.A. No. 18 stipulates that the minimum safe manning level for the vessel is 2 crew members, and the AR crewed the vessel to this level.
As of late 2022, TC is requesting information from ARs regarding how a person-overboard emergency would be dealt with. However, because this requirement is not prescribed it can be applied inconsistently, as is the case with the SMD issued to one of the A.P.A. No. 18’s sister ships, and the SMDs issued to other pilot boats across the country. As this and other TSB investigationsFootnote 61 demonstrate, insufficient crew affects crews’ ability to effectively carry out emergency duties even when manning levels are in compliance with SMDs.
Finding as to risk
If safe manning criteria do not consider person overboard and incapacitation emergencies, and those criteria are not consistently applied, there is a risk that vessels with low minimum safe manning levels will not have sufficient crew to effectively respond to an emergency situation.
2.3 Fatigue management
Given the performance impairments that occur when a person is fatigued, it is critical that organizations manage fatigue effectively. At the time of the occurrence, Canship’s fatigue policy included limitations for work and rest that were based on the requirements of the MPR. The work schedule for the crew of the A.P.A No. 18 is in 1 of 2 shift formats: 7 days on duty and 14 days off, or 14 days on duty and 7 days off, with a requirement to return to the vessel within 15 minutes of being called while on duty.
The risk of impairment from fatigue is increased by long shift durations; for example, working a maximum of 18 hours before receiving a mandatory 6 hours off. While 6 hours off is prescribed following an 18-hour shift, restorative sleep may be difficult for crew to obtain or may not occur because of the irregular and unpredictable timing of the rest period. As well, activities other than sleep need to be performed during the 6-hour break, such as travel and eating.
In the A.P.A No. 18’s work schedule, the risk of impairment from fatigue is greatest for the individuals working the 14 days on, 7 days off shift due to the longer amount of time that the crew are on shift and the 15-minute call back requirement for 24 hours a day, 14 days in a row.
The MPR establishes the minimum hours of rest for seafarers, and work schedules that follow these requirements can introduce a number of fatigue risk factors such as
- acute sleep disruption from early and late pilot transfers;
- chronic sleep disruption related to the irregular and unpredictable schedule;
- continuous wakefulness; and
- circadian rhythm effects due to the irregular and unpredictable work schedule, and occasionally working during the nighttime circadian trough.
The issue of inadequate fatigue management is not limited to the A.P.A. No. 18. The TSB Watchlist 2022 has identified that there is currently no mandatory requirement in the MPR for companies to have comprehensive fatigue awareness training or a fatigue management plan. Given the long hours and irregular and unpredictable schedules involved in marine pilotage operations, there is a need for greater awareness of the risks associated with fatigue and effective strategies to mitigate those risks.
Finding as to risk
Without effective fatigue risk management, crews working irregular and unpredictable work schedules, with long hours, may be at increased risk of performance impairments due to fatigue.
2.4 Servicing and maintenance of personal flotation devices
PFDs are vital pieces of drowning prevention equipment in the marine industry. To be functional, PFDs must be maintained according to the manufacturer’s instructions. The maintenance, servicing, and inspection requirements for PFDs are different depending on whether they are inflatable or inherently buoyant. Maintenance requirements for inflatable PFDs, such as the 1 used in this occurrence, are more complex than other PFD types.
Inflatable PFDs not being maintained according to the manufacturer’s instructions is a known and persistent hazard. As the United States Coast Guard and TC safety messages indicate, it is common for the functionality of inflatable PFDs to be impaired when they have not been maintained in accordance with the manufacturer’s instructions.
Although PFDs do not require third-party servicing, due to the complex nature of their maintenance, PFD owners sometimes send them to a third party. Not all third parties have the same certifications for PFD servicing and maintenance; to ensure PFDs are being maintained according to the manufacturer’s instructions, PFD owners and users need to be aware of third-party accreditation. Further, even when serviced by a third party, there are still critical elements in the manufacturer’s instructions that must be completed by the user. In this occurrence, Canship had its PFDs serviced by a third party with the expectation that they would be serviced to the manufacturer’s instructions.
The occurrence PFD was rearmed and inspected in April 2022 by a third party. The third party used its own generic checklist, which included a 1-hour leak test; this test was performed with the expectation that all deficiencies with any PFD type would be identified in that testing timeframe.
Because PFD rearming, repacking and inspection was delegated to a third party, it is likely that there was an expectation on the part of Canship that additional maintenance as detailed in the manufacturer’s instructions would not be required, although Canship policy did require personal protective equipment to be maintained according to manufacturer’s instructions. Since inspections by the masters were conducted regularly, it is likely there was an expectation on the part of the A.P.A. No. 18’s crew that the occurrence PFD would be ready for use and not require pre-use inspection as detailed in the manufacturer’s instructions. In addition, the occurrence PFD was shared among the deckhands who worked on board the vessel. When a piece of personal protective equipment is shared, the responsibility for it is shared as well, which may result in pre-use inspections not being completed by each user as required. Critical elements of the manufacturer’s instructions, such as pre-use inspections and air-leak testing by users, were not completed on the occurrence PFD.
The TSB laboratory tested the occurrence PFD and others under various conditions. During testing, the separation of the inflator cap and body occurred only when the manufacturer’s instructions were not followed. The investigation could not determine when the separation of the inflator cap and body on the occurrence PFD occurred; however, the investigation did determine it was not identified as a deficiency. Air-leak tests done at regular intervals are designed to identify leaks, and a general awareness and hands-on training in user PFD maintenance, according to the manufacturer’s instructions, is a best practice that increases the likelihood of deficiencies being identified. Because the deficiency was not identified, the PFD was used on the night of the occurrence.
Finding as to risk
Inflatable PFDs require servicing that must be done in accordance with the manufacturer’s instructions. When all persons involved in inflatable PFD inspection and maintenance are not aware of or trained with the manufacturer’s instructions, there is a risk that deficiencies will not be identified and corrected, which may result in crew using PFDs that are damaged or non-functional.
2.5 Personal flotation device failure
Given that conducting pilot transfers includes a high risk of going overboard, Canship and APA have implemented mitigation measures to reduce this risk, such as requiring that all crew and pilots wear a PFD when on deck. Research has shown that correctly wearing lifejackets and PFDs reduces the risk of cold shock on a person who is unexpectedly immersed in cold water, which effectively gives rescuers more time to retrieve that person. However, when an inflatable PFD fails to inflate, the protection and additional time for retrieval is lost. The PFD worn by the deckhand did not provide buoyancy in this occurrence.
The occurrence PFD was thoroughly examined and tested by the TSB laboratory where it was found that the inflator cap and inflator body were separated. Inflatable PFDs like the one used in this occurrence will not inflate when the cap and body are separated. Since the inflator cap and body must be mated to seal this inflatable PFD's bladder, any attempts to inflate the occurrence PFD using the manual pull tab or oral inflation tube would have been unsuccessful. The TSB laboratory also found that the occurrence PFD’s CO2 cartridge was not punctured even though the cap was activated.
Although the investigation could not determine exactly when the inflator cap and body separation occurred, testing revealed that the separation happened prior to the occurrence; the inflator cap and body were separated at some point during or after the PFD’s last servicing.
Finding as to causes and contributing factors
The occurrence PFD’s inflator cap and inflator body were separated, which prevented it from inflating and providing buoyancy. The PFD’s failure to inflate reduced the likelihood of the deckhand’s survival while he was immersed in cold water.
2.6 Communication of safety information and safety management
An effective safety management system (SMS) is not just a set of documents, but relies on a culture of 2-way communication of safety information to identify and mitigate hazards in the work environment. Operational safety information can be communicated to management through hazard reporting, near-miss reporting, debriefing from drills or exercises, occupational health and safety committee minutes, non-compliance reports, and audit reports. Once hazards are identified at the operational level and communicated, controls can be put in place to reduce risks, which can then be communicated back to the operational level as implemented training, procedure, audits, and inspections. Gaps in communication can result in operating with unmitigated hazards.
The investigation found that opportunities for operational-level safety information to be communicated and then integrated into Canship’s SMS were missed. The following are examples of how the flow of safety information was affected from the operational level for integration into Canship’s SMS:
- Reporting procedures are found in Canship’s SMS manual which is considered by crew to be less relevant for pilot boat operations.
- Canship’s SMS includes information about known hazards and how to identify them. However, no feedback, lessons learned, or hazards were recorded in the safety committee minutes between January 2022 and September 2022.
- Issues associated with the use of the wire and tether system as designed and installed were not formally reported or mitigated.
- Person-overboard drills as practised did not reflect typical conditions, and the hazards associated with low crewing levels were not formally reported through Canship’s SMS for action and follow-up.
- APA, in the last inspection before the occurrence, found that the person-overboard retrieval system was difficult for 1 person to use; this safety-related information from APA was not formally actioned, in part because this safety-related information was not received by Canship.
A number of factors underly this ineffective flow of safety information. One factor is the design of the SMS and its application to the A.P.A. No. 18. Canship voluntarily applies its tanker and cargo ship SMS to pilot boat operations, with some pilot boat–specific procedures originating from APA; however, this results in the A.P.A. No. 18 being subject to an SMS that does not completely take into account its day-to-day operations. The Canship SMS is complex; it is spread across multiple documents, only 1 of which is specific to pilot boat operations. The Canship SMS has large parts that are not relevant to pilot boat operations, and it focuses on compliance with regulation. Also, key aspects of the Canship SMS, which enable communication of safety information, such as hazard identification, incident reporting, emergency response, and drills and exercise conduct, are found in Canship SMS manuals which are considered by crew to be secondary for pilot boat operations.
Another factor affecting the flow of safety information is the model used to operate the A.P.A. No. 18. Although APA is the owner of the occurrence vessel and it conducts risk assessments and annual inspections, it does not manage day-to-day operations on the A.P.A. No. 18. Even though APA has safety programs for pilot boats that it owns and manages that are relevant to pilot boat risk, many of these programs are not incorporated into Canship’s SMS. In addition, the on-the-job-training guidance that Canship uses to familiarize new crew members on the A.P.A. No. 18 was developed by APA and references programs that are not contained within Canship’s SMS documentation, which can confuse crew members of the A.P.A. No. 18, who participate in Canship’s SMS.
The investigation identified known hazards that were not reported through Canship’s SMS. The hazards associated with the design of the wire and tether system, inflatable PFDs, and a low crewing level were known at the operational level and through APA inspection, but were not actioned by various safety management processes in place. Because the safety management processes of continuous improvement did not support communication of safety information across hierarchical levels, many of these hazards existed with ineffectual controls in place.
Finding as to risk
If a company’s SMS does not facilitate the flow of safety information from the operational level to management, there is a risk of vessels operating with hazards that are known but without adequate defences.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The design of the wire and tether system and the way it was installed on board the A.P.A. No. 18 prevented the deckhands from being continuously connected to the wire as they moved between the fixed stairs and bow of the vessel.
- This system design and installation necessitated an adapted practice of disconnecting the tether from the wire while transitioning from the side to the front of the wheelhouse, which contributed to the occurrence deckhand being untethered and subsequently falling overboard.
- The design of the vessel combined with its level of emergency preparedness made it practically impossible for the master alone to retrieve the deckhand from the water. Consequently, the deckhand was immersed in cold water for a prolonged period of time.
- The occurrence personal flotation device’s (PFD) inflator cap and inflator body were separated, which prevented it from inflating and providing buoyancy. The PFD’s failure to inflate reduced the likelihood of the deckhand’s survival while he was immersed in cold water.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If safe manning criteria do not consider person overboard and incapacitation emergencies, and those criteria are not consistently applied, there is a risk that vessels with low minimum safe manning levels will not have sufficient crew to effectively respond to an emergency situation.
- Without effective fatigue risk management, crews working irregular and unpredictable work schedules, with long hours, may be at increased risk of performance impairments due to fatigue.
- Inflatable personal flotation devices (PFDs) require servicing that must be done in accordance with the manufacturer’s instructions. When all persons involved in inflatable PFD inspection and maintenance are not aware of or trained with the manufacturer’s instructions, there is a risk that deficiencies will not be identified and corrected, which may result in crew using PFDs that are damaged or non-functional.
- If a company’s safety management system does not facilitate the flow of safety information from the operational level to management, there is a risk of vessels operating with hazards that are known but without adequate defences.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- The A.P.A. No. 18 had not undergone a maritime occupational health and safety inspection in the 5 years before the occurrence.
- There is no mandatory post-occurrence drug and alcohol testing in the marine industry for Canadian crews involved in occurrences.
- The deckhand was subject to multiple fatigue risk factors such as acute sleep disruption, chronic sleep disruption, continuous wakefulness, circadian rhythm effects, and likely was fatigued at the time of the occurrence.
- The manual pull tab on the occurrence personal flotation device was tucked in where it could not be accessed by the user.
4.0 Safety action
4.1 Safety action taken
4.1.1 TSB
On 21 February 2023, the TSB issued a safety advisory letterFootnote 62 to the Operations Manager of Canship Ugland Ltd. and to the Chief Operating Officer of the Atlantic Pilotage Authority (APA). This letter referred to Transport Canada’s Ship Safety Bulletin 12/2019, which highlights the need to inspect and service inflatable lifejackets and personal flotation devices (PFDs) regularly and in accordance with manufacturers’ instructions. In response, the APA shared the safety advisory letter with all employees and pilot boat contractors, as well as amongst other pilotage authorities.
4.1.2 Atlantic Pilotage Authority
As a result of the occurrence, the APA convened a special occupational health and safety meeting on 05 October 2022 and the following was immediately put into place:
- The wire and tether system on the A.P.A No. 18 and sister vessels (the A.P.A No. 1 and the A.P.A No. 20) were modified; lines were added to areas of the vessels that had none before, and the wires along the sides of the wheelhouses were loosened.
- A 2-tether system was implemented.
- A third crew member was added to the A.P.A. No. 18’s complement.
- The A.P.A. No. 18’s fixed steps were upgraded with gratings for added grip.
- The A.P.A. No. 18 crew were instructed to set the person-overboard retrieval system prior to leaving the harbour.
- Mandatory inspection and testing of inflatable PFDs.
Following the meeting on 05 October 2022, the APA also implemented the following:
- A fleet-wide review of tethering systems, with hardware upgrades when possible to ensure tethering can occur at all times (including the upgrade of safety rail for the A.P.A. No. 18 and sister ships).
- Field testing of PFDs with wind and waves, as well as employee familiarization of PFDs and lifejackets.
- A list of APA–approved PFDs, tethers, and harnesses was compiled.
- A fleet-wide review of retrieval systems with upgrades provided when possible, including electric winches with a single whip for side-arm davits.
- Increased frequency of person-overboard drills in more realistic conditions.
- The conduct of person-overboard drills with 1 and 2 persons.
- The procurement of person-overboard danbuoys for the fleet.
- The assessment of existing exterior lighting on pilot boats and the installation of improved exterior lighting where required.
- Issuing most employees with SOLAS–approved inflatable lifejackets with twin inflation chambers, instead of PFDs.
4.1.3 Canship Ugland Ltd.
As a result of the occurrence, Canship Ugland Ltd. put the following into place:
- The use of double lanyards when using the tethering system.
- The installation of an electric winch on the A.P.A. No. 18’s recovery system.
- A new safety committee form.
- A review of operating procedures and the development of vessel-specific risk assessments for pilot transfer operations.
- The increased frequency of person-overboard drills in a variety of environmental conditions.
- The replacement of shepherd hooks for person-overboard recovery with lighter, extendable hooks.
- The procurement of SOLAS–approved Spinlock double-cannister PFDs. Annual service for the PFDs is provided by a third-party contractor.
- The development and implementation of a Safety Equipment Inspection and Maintenance regime.
- A vessel deficiency list will be sent to the Superintendent weekly, instead of monthly. All deficiencies will be added to DocMap for tracking and closure.
- The installation of a safety rail system on the A.P.A. No. 18. The rail systems on other pilot boats will be modified if needed.
- The improvement of heat-tracing capabilities in the safety rail systems on all pilot boats; ensure in working order.
- The outfitting of all crew members with personal safety kits that include a harness, a lanyard, a PFD, a helmet, and an automatic identification system (AIS) unit.
- A personal protective equipment checklist for crew members of the A.P.A. No. 18.
- A personal protective equipment reference guide for crew members of the A.P.A. No. 18.
- The procurement of person-overboard danbuoys for all pilot boats, as an additional means of flotation for person-overboard emergencies.
- The improvement of outside lighting and person-overboard lighting on board the A.P.A. No. 18 for better visibility during nighttime operations.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Mustang Survival Corp.’s instructions for PFD inspection, care, and maintenance

READINESS CHECKLIST
Check your PFD and ensure all of the checkpoints listed below are true before use.
- Single point status indicator is green (Fig. 2 or 2a).
- Ensure the current date is not past the date on the inflator. If it is, replace the inflator (see Re-arming Your PFD, p. 9).
- Ensure both zipper stops are in place under Velcro™ tab (Fig. 1).
- All zippers, Velcro™, and waist buckle are securely fastened.
- Oral inflation cap is in the stowed position (Fig. 7).
- PFD is not twisted.
- Ensure the inflation pull-tab is hanging on the outside (Fig. 31).
- No rips, tears, excessive abrasion, or holes; all seams are securely sewn; and the cover, straps, and hardware are still strong.
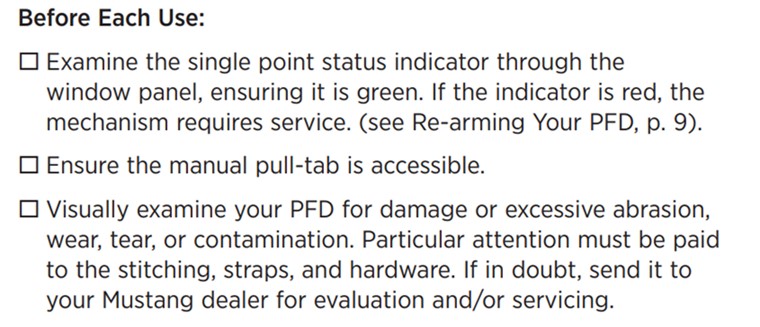
CARE AND MAINTENANCE INSTRUCTIONS
1. Before each use:
- Examine the single point status indicator through the window panel, ensuring it is green. If the indicator is red, the mechanism requires service. (See Re-arming Your PFD, p. 9).
- Ensure the manual pull-tab is accessible.
- Visually examine your PFD for damage or excessive abrasion, wear, tear, or contamination. Particular attention must be paid to the stitching, straps, and hardware. If in doubt, send it to your Mustang dealer for evaluation and/or servicing.
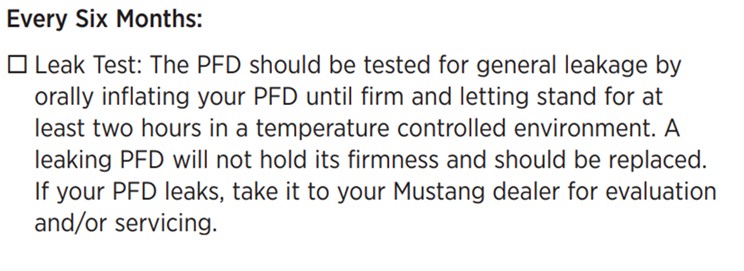
CARE AND MAINTENANCE INSTRUCTIONS
2. Every Six Months:
- Leak Test: The PFD should be tested for general leakage by orally inflating your PFD until firm and letting stand for at least two hours in a temperature controlled environment. A leaking PFD will not hold its firmness and should be replaced. If your PFD leaks, take it to your Mustang dealer for evaluation and/or servicing.
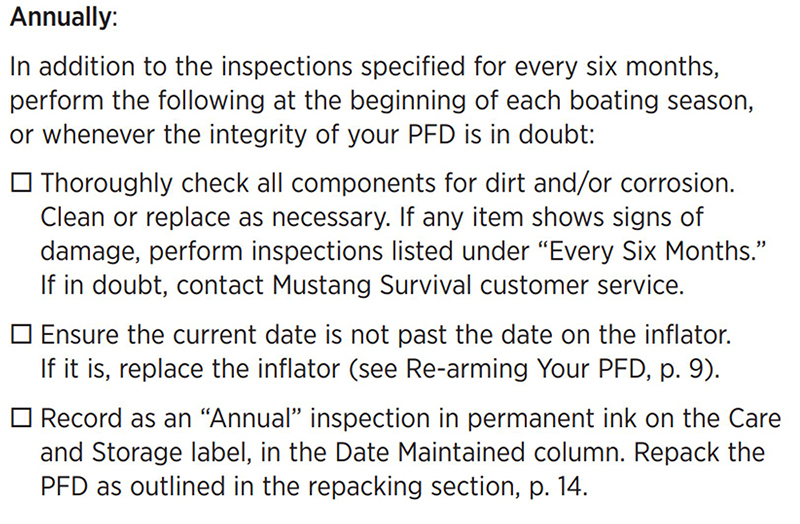
CARE AND MAINTENANCE INSTRUCTIONS
3. Annually:
In addition to the inspections specified for every six months, perform the following at the beginning of each boating season, or whenever the integrity of your PFD is in doubt:
- Thoroughly check all components for dirt and/or corrosion. Clean or replace as necessary. If any item shows signs of damage, perform inspections listed under “Every Six Months.” If in doubt, contact Mustang Survival customer service.
- Ensure the current date is not past the date on the inflator. If it is, replace the inflator (see Re-arming Your PFD, p. 9).
- Record as an “Annual” inspection in permanent ink on the Care and Storage label, in the Date Maintained column. Repack the PFD as outlined in the repacking section, p. 14.
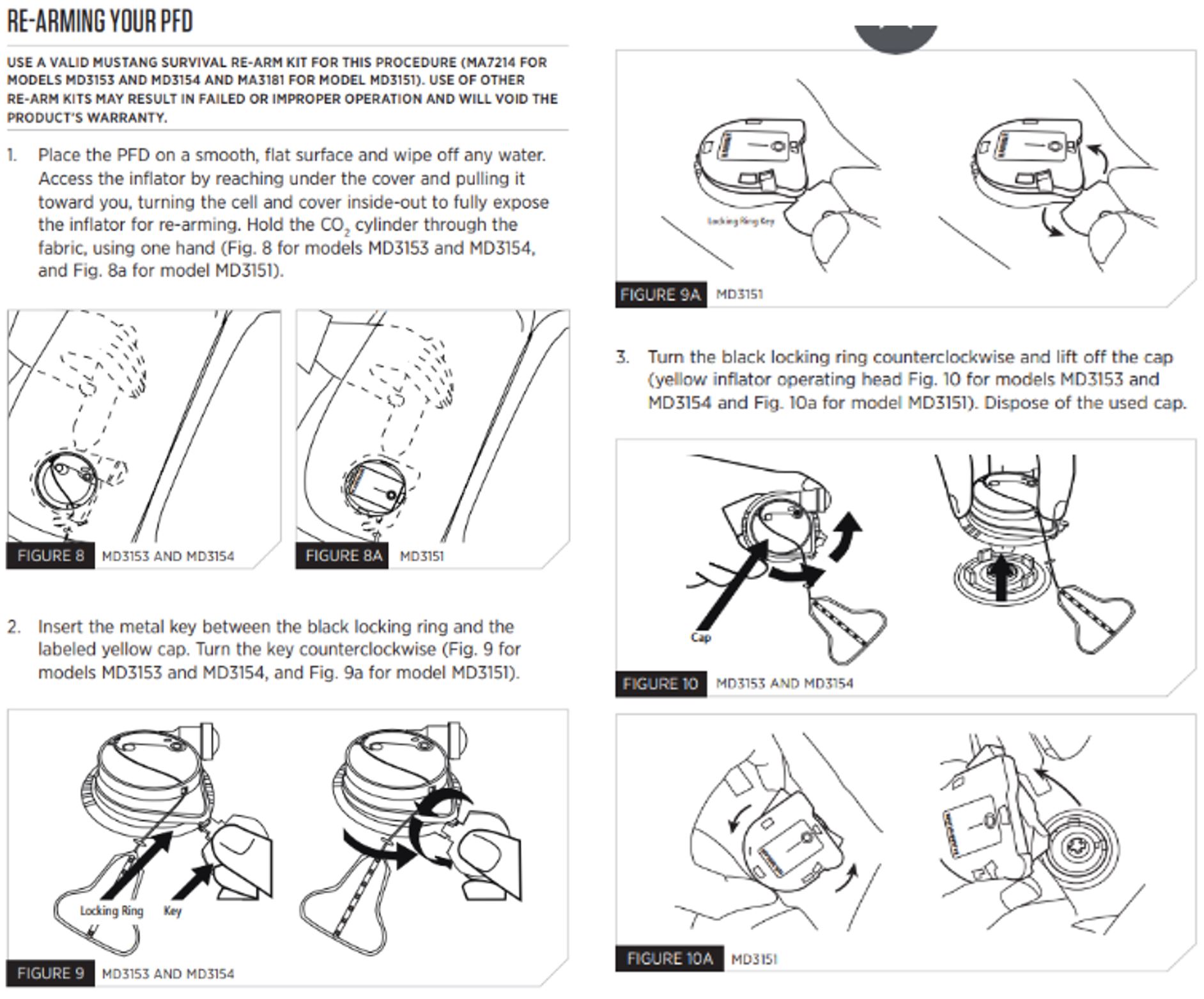
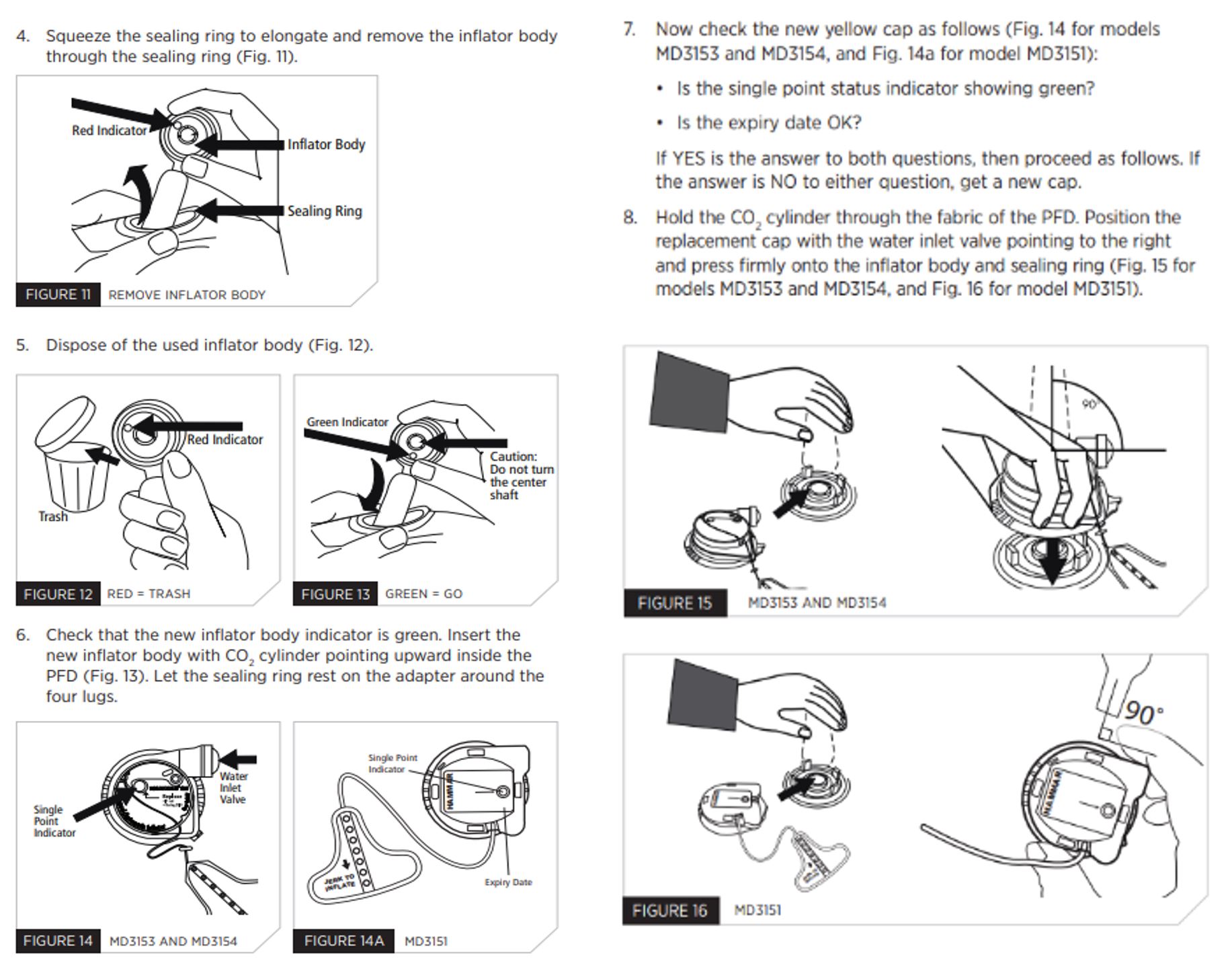
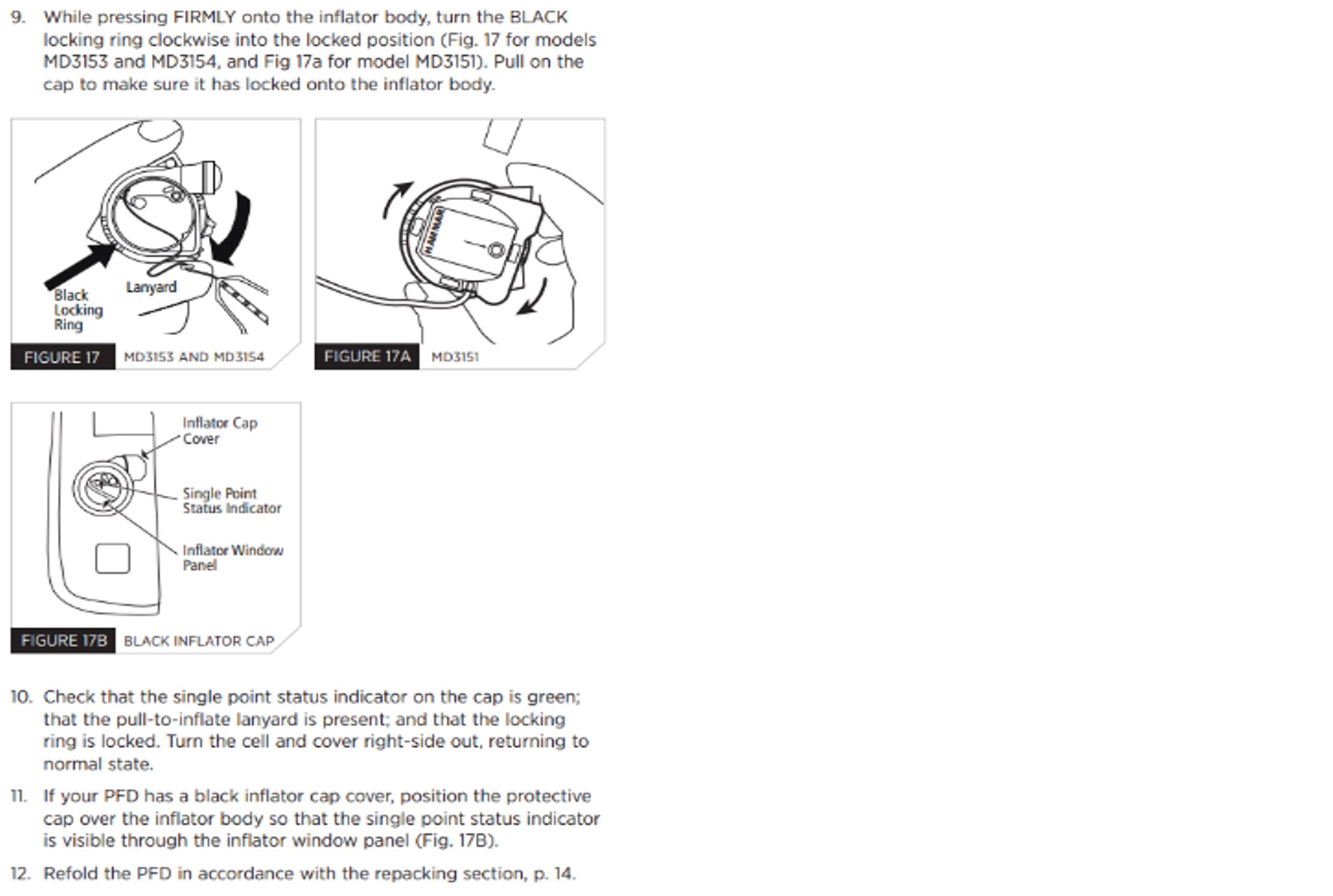
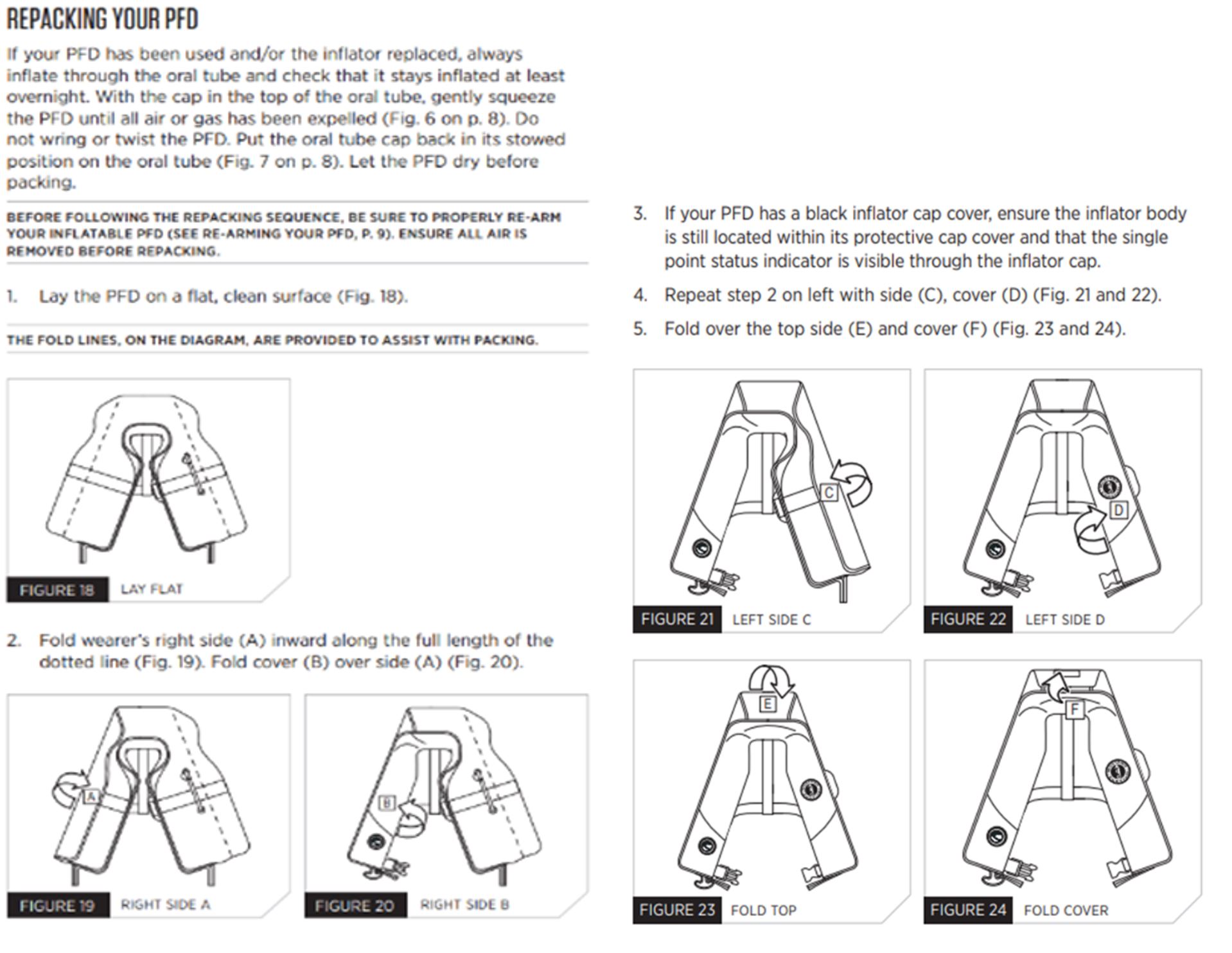
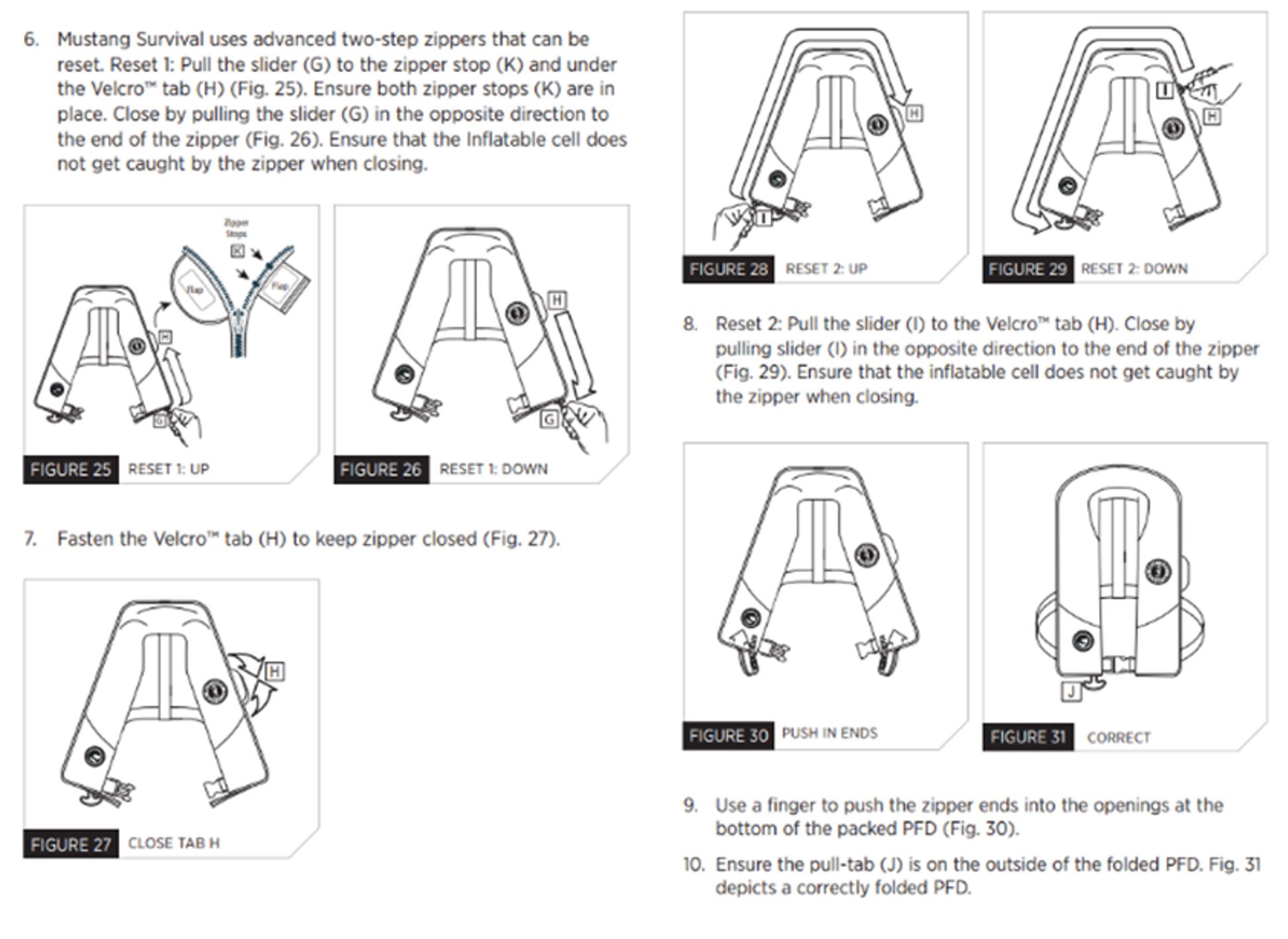
RE-ARMING YOUR PFD
USE A VALID MUSTANG SURVIVAL RE-ARM KIT FOR THIS PROCEDURE (MA7214 FOR MODELS MD3153 AND MD3154 AND MA3181 FOR MODEL MD3151). USE OF OTHER RE-ARM KITS MAY RESULT IN FAILED OR IMPROPER OPERATION AND WILL VOID THE PRODUCT’S WARRANTY.
1. Place the PFD on a smooth, flat surface and wipe off any water. Access the inflator by reaching under the cover and pulling it toward you, turning the cell and cover inside-out to fully expose the inflator for re-arming. Hold the CO2 cylinder through the fabric, using one hand (Fig. 8 for models MD3153 and MD3154, and Fig. 8a for model MD3151).
2. Insert the metal key between the black locking ring and the labeled yellow cap. Turn the key counterclockwise (Fig. 9 for models MD3153 and MD3154, and Fig. 9a for model MD3151).
3. Turn the black locking ring counterclockwise and lift off the cap (yellow inflator operating head Fig. 10 for models MD3153 and MD3154 and Fig. 10a for model MD3151). Dispose of the used cap.
4. Squeeze the sealing ring to elongate and remove the inflator body through the sealing ring (Fig. 11).
5. Dispose of the used inflator body (Fig. 12).
6. Check that the new inflator body indicator is green. Insert the new inflator body with CO2 cylinder pointing upward inside the PFD (Fig. 13). Let the sealing ring rest on the adapter around the four lugs.
7. Now check the new yellow cap as follows (Fig. 14 for models MD3153 and MD3154, and Fig. 14a for model MD3151):
• Is the single point status indicator showing green?
• Is the expiry date OK?
If YES is the answer to both questions, then proceed as follows. If the answer is NO to either question, get a new cap.
8. Hold the CO2 cylinder through the fabric of the PFD. Position the replacement cap with the water inlet valve pointing to the right and press firmly onto the inflator body and sealing ring (Fig. 15 for models MD3153 and MD3154, and Fig. 16 for model MD3151).
9. While pressing FIRMLY onto the inflator body, turn the BLACK locking ring clockwise into the locked position (Fig. 17 for models MD3153 and MD3154, and Fig 17a for model MD3151). Pull on the cap to make sure it has locked onto the inflator body.
10. Check that the single point status indicator on the cap is green; that the pull-to-inflate lanyard is present; and that the locking ring is locked. Turn the cell and cover right-side out, returning to normal state.
11. If your PFD has a black inflator cap cover, position the protective cap over the inflator body so that the single point status indicator is visible through the inflator window panel (Fig. 17B).
12. Refold the PFD in accordance with the repacking section, p. 14.
REPACKING YOUR PFD
If your PFD has been used and/or the inflator replaced, always inflate through the oral tube and check that it stays inflated at least overnight. With the cap in the top of the oral tube, gently squeeze the PFD until all air or gas has been expelled (Fig. 6 on p. 8). Do not wring or twist the PFD. Put the oral tube cap back in its stowed position on the oral tube (Fig. 7 on p. 8). Let the PFD dry before packing.
BEFORE FOLLOWING THE REPACKING SEQUENCE, BE SURE TO PROPERLY RE-ARM YOUR INFLATABLE PFD (SEE RE-ARMING YOUR PFD, P. 9). ENSURE ALL AIR IS REMOVED BEFORE REPACKING.
1. Lay the PFD on a flat, clean surface (Fig. 18).
THE FOLD LINES, ON THE DIAGRAM, ARE PROVIDED TO ASSIST WITH PACKING.
2. Fold wearer’s right side (A) inward along the full length of the dotted line (Fig. 19). Fold cover (B) over side (A) (Fig. 20).
3. If your PFD has a black inflator cap cover, ensure the inflator body is still located within its protective cap cover and that the single point status indicator is visible through the inflator cap.
4. Repeat step 2 on left with side (C), cover (D) (Fig. 21 and 22).
5. Fold over the top side (E) and cover (F) (Fig. 23 and 24).
6. Mustang Survival uses advanced two-step zippers that can be reset. Reset 1: Pull the slider (G) to the zipper stop (K) and under the Velcro™ tab (H) (Fig. 25). Ensure both zipper stops (K) are in place. Close by pulling the slider (G) in the opposite direction to the end of the zipper (Fig. 26). Ensure that the Inflatable cell does not get caught by the zipper when closing.
7. Fasten the Velcro™ tab (H) to keep zipper closed (Fig. 27).
8. Reset 2: Pull the slider (I) to the Velcro™ tab (H). Close by pulling slider (I) in the opposite direction to the end of the zipper (Fig. 29). Ensure that the inflatable cell does not get caught by the zipper when closing.
9. Use a finger to push the zipper ends into the openings at the bottom of the packed PFD (Fig. 30).
10. Ensure the pull-tab (J) is on the outside of the folded PFD. Fig. 31 depicts a correctly folded PFD.
Appendix B – Mustang Inflatable PFD Re-arm Kit “C” instructions